
Potential Health Benefits of Tesofensine
Tesofensine offers a range of potential benefits, including promoting weight loss, improving cognitive health, enhancing mood, regulating blood sugar levels, boosting energy, addressing sexual dysfunction, treating eating disorders, managing ADHD, improving sleep quality, and aiding in the fight against alcohol addiction.
- Promotes weight loss [6-23]
- Improves cognitive health [24-32]
- Improves mood [33-35]
- Improves blood sugar levels [36-38]
- Increases energy levels [35, 39]
- Treats sexual dysfunction [35, 40]
- Treats eating disorders [8, 41-45]
- Treats attention-deficit/hyperactivity disorder (ADHD) [46-49]
- Improves sleep quality [50-57]
- Fights alcohol addiction [58-62]
Key Takeaways of Tesofensine Guide 2023
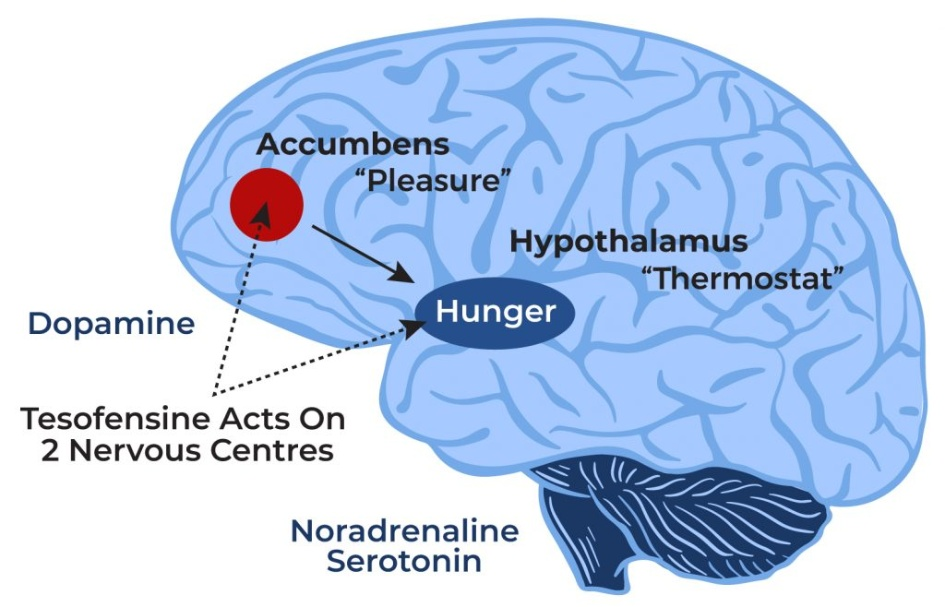
- Tesofensine is a triple re-uptake inhibitor that increases the levels of three neurotransmitters in the brain: Serotonin, norepinephrine, and dopamine.
- Tesofensine benefits include weight loss, fat loss, increased energy levels, improved sex drive, better erections, improved mood, improved memory, improved concentration, better sleep, and better blood glucose levels by improving insulin sensitivity and glucose metabolism. Tesofensine causes a significant increase in weight loss and fat loss by reducing appetite, increasing resting energy expenditure (ie increasing metabolism and calories burned), increasing fat oxidation, and reducing fat tissue.
- Tesofensine is one of the most effective, powerful weight-loss medications available on the market. Studies have shown more weight loss with higher tesofensine doses was up to 1 mg. A clinical study found that participants receiving tesofensine at doses of 0.25 mg, 0.5 mg, and 1.0 mg in conjunction with a prescribed diet for 6 months had a mean weight loss of 4.5%, 9.2%, and 10.6%. Comparatively, patients in this study treated with a placebo only lost an average of 2% of their body weight. There was a 4-point drop in BMI in a period of 24 weeks in those treated with 0.5 mg and 1 mg.
- Tesofensine has been shown to have a good safety profile and was well tolerated although an increased number of adverse events (e.g., increased heart rate and blood pressure) were observed in the higher dose groups of 0.5 mg and 1.0 mg. Blood pressure and heart rate were increased by 1–3 mmHg and up to 8 bpm, respectively. Other side effects of Tesofensine may include dry mouth, headache, nausea, insomnia, diarrhea, and constipation. Although some studies show it may have anti-anxiety properties, some people may experience an increase in anxiety levels. Side effects are dose-dependent and are more significant when using higher doses.
- The tesofensine dosage range used in studies was 0.25 mg to 1 mg. The weight loss of 9.2% in the 0.5 mg tesofensine dose vs 10.6% in those using the 1 mg tesofensine dose may not justify the dose-dependent increases in side effects. Based on this, the best tesofensine dose for most patients would be 0.5 mg or lower. You should consult your weight loss expert doctor to determine if tesofensine is right for you and the dosage should be custom tailored.
- Only purchase tesofensine through a legally accredited US pharmacy prescribed by your expert weight loss doctor custom tailored for you. Do not buy tesofensine online because there are no testing requirements or regulations of these products to guarantee that it is even tesofensine, that is high-quality tesofensine, and that it is pure and does not contain any harmful chemicals. Consult with an expert weight loss doctor who has a lot of experience prescribing tesofensine and understands its potential side effects, contraindications, and drug interactions. A thorough medical history and exam should be completed along with the appropriate blood work. Caution: Tesofensine is a prescription medication that can cause side effects and it may not be a good weight loss option for you based on your medical history, blood work, or current medication use. An expert weight loss doctor will help you determine this. Tesofensine is not a supplement and should not be purchased online as a supplement. It is also very unwise for humans to use this medication by purchasing it online on websites that sell it with the legal loophole that it is being sold “for research purposes only”.
What is Tesofensine?
Tesofensine (NS2330) is a serotonin–noradrenaline–dopamine reuptake inhibitor or also known as a triple reuptake inhibitor, which means that it inhibits the reabsorption of the neurotransmitters (brain chemicals) serotonin, norepinephrine, and dopamine. This process increases the levels of these neurotransmitters. The therapeutic benefits of tesofensine are attributed to this effect because each of these neurotransmitters exerts an important function at different locations in the brain. Tesofensine peptide has been investigated in clinical trials for its use in medical weight loss.
How Does Tesofensine Work?
Tesofensine works by boosting the levels of brain chemicals (neurotransmitters) such as dopamine, norepinephrine, and serotonin. Dopamine is associated with the regulation of motor function, mood, motivation, reward, cognitive function, and reproductive behaviors. Norepinephrine increases the force of the contraction of the skeletal muscle and the heart to ensure optimal body function. Serotonin is responsible for the regulation of mood, memory, sleep, and appetite.
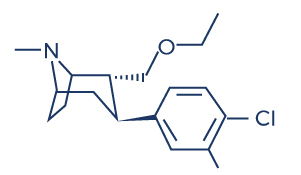
Chemical Structure of Tesofensine
Research Studies/Clinical Trials on Tesofensine
A. Promotes Weight Loss

Optimal dopamine levels have a positive impact on appetite regulation, metabolism, and motivation. On the other hand, dopamine deficiency can promote weight gain. Dopamine suppresses appetite, reduces cravings, and lowers calorie consumption. It also boosts metabolism by increasing thermogenesis, leading to improved calorie burning and increased energy expenditure. Moreover, dopamine enhances motivation and satisfaction, which helps produce feelings of satiety.
Tesofensine is widely known as a weight loss drug. Researchers believe that tesofensine may help treat obese and overweight patients because it boosts the levels of dopamine in the brain. A deficiency in this neurotransmitter has been shown to be linked with overeating and obesity. [1-5]
Fat oxidation, also known as lipid oxidation or fat burning, refers to the process by which stored fat is broken down and converted into usable energy within the body. There are some mechanisms by which tesofensine may contribute to increased fat burning such as increased metabolism, appetite suppression, and modulation of neurotransmitters. As an appetite suppressant, it may indirectly promote increased physical activity which leads to increased fat oxidation. When combined with lifestyle modification, the body responds well to the effects of tesofensine.
Discover the Power of Peptides for Weight Loss! Learn how peptides can support your weight loss journey and improve your overall health. Explore our comprehensive guide on peptides for weight loss at Genemedics and take the first step towards a healthier, happier you!
Clinical trials involving tesofensine have evaluated its efficacy and safety in promoting weight loss:
- The results of phase III trials such as the 2018 phase 3 Viking study showed that obese participants who received both doses of oral tesofensine (0.25 and 0.50 mg once daily) had statistically and clinically significant reductions in weight with low incidence of adverse events at week 24. [6]
- The results of clinical trials such as the Phase II b trial (TIPO-1) showed that obese patients lost an average of 12.8 kg on the 1 mg dose, 11.3 kg on the 0.5 mg dose, and 6.7 kg on the 0.25 mg dose of tesofensine (dose-dependent increase), and showed no statistically significant increases in systolic or diastolic blood pressure, compared with a 2.2 kg loss in the placebo group. [7] The 24-hour fat oxidation (fat burning) also increased by 15% and there was a reduction in protein oxidation (the breakdown of protein due to the presence of reactive oxygen species).
- In the TIPO-2 trial, tesofensine administration in obese individuals reduced their desire to eat and increased their satiety levels after 14 days of treatment. [8]
- In patients with obesity, tesofensine treatment at varying doses (0.25 mg, 0.5 mg, or 1.0 mg) resulted in statistically significant and clinically relevant weight reductions with positive effects on energy balance and appetite. The patients were also able to increase their physical activity gradually, which led to improved quality of life. Significant results were seen in the highest dose groups. [9]
- In obese participants, tesofensine administration at a dose of 0.5 mg for 26 weeks produced weight reductions twice that of anti-obesity agents such as sibutramine or rimonabant. [10]
- In overweight patients, tesofensine administration for 24 weeks is associated with enhanced appetite suppression and significant weight reductions. [11]
- In phase II clinical trials with tesofensine in obese individuals, significant reductions in weight, body fat, and waist circumference were observed without any adverse side effects. [12]
- In obese individuals, long-term tesofensine supplementation was well-tolerated and resulted in statistically significant and clinically relevant weight loss. [13]
- In patients with Parkinson’s or Alzheimer’s disease, tesofensine administration once daily for 14 weeks induced weight loss of approximately 4%, which is similar to that of sibutramine. [14]
- In healthy males, multiple administrations of tesofensine at doses of 0.125–1 mg resulted in the following positive results: increased dopamine levels and appetite suppression. [15]
- In diet-induced obese rats, tesofensine administration resulted in appetite suppression and weight loss with a reversal of low forebrain dopamine levels. [16-17]
- In a rat model of diet-induced obesity (DIO), administration of tesofensine (2.0 mg/kg, s.c.) for 16 days significantly reduced body weights. [18]
- In diet-induced obese rats, tesofensine treatment at 2 mg/kg for 28 days decreased food consumption and produced dramatic weight losses while preventing weight gain. [19]
- In 203 obese persons, tesofensine 0.5 mg produced a weight loss twice that of currently approved anti-obesity medications. [20]
- In obese participants, tesofensine administration resulted in a 10% average weight loss in 24 weeks. The patients were also able to increase their physical activity gradually after the treatment. [21]
- A study showed that tesofensine showed a more significant effect on body weight than that of currently approved anti-obesity drugs. [22]
- In obese patients, tesofensine in combination with an energy-restricted diet effectively reduced the weight of the subjects. [23]
B. Improves Cognitive Health

Research indicates that tesofensine helps preserve cognitive health by indirectly potentiating cholinergic neurotransmission, which is a process whereby nerve cells relay messages to each other. [24] This has been proven to have beneficial effects on various areas in the central nervous system and cognitive health including learning, memory, and thinking skills. This suggests that tesofensine may be used in the treatment of brain disorders such as Alzheimer’s and Parkinson’s disease. The following studies support this effect:
- The first results of two small 4-week phase IIa clinical trials performed in patients with mild Alzheimer’s disease (AD) showed that tesofensine treatment induced significant improvement in cognitive function, indicating the need for phase III trials. [25-26]
- A growing body of research indicates that obesity is a major risk factor for cognitive impairment, especially in the older population. [27-30] With its anti-obesity effect, tesofensine may help protect against cognitive impairment.
- In a mouse model of Alzheimer’s disease, tesofensine administration decreased the brain concentrations of amyloid beta, which are abnormal protein aggregates and is the causative agent of the disease. [31]
- In patients with advanced Parkinson’s disease and motor fluctuations, low-dose tesofensine improved activities of daily living and motor function. [32]
C. Improves Mood

The mood centers of the central nervous system have also been shown to be positively affected by tesofensine. Sustained treatment with tesofensine has been shown to improve overall mood through its antidepressant effect. Studies show that tesofensine affects mood by:
- Increasing the levels of brain-derived neurotrophic factor (BDNF), thereby triggering an antidepressant effect. [33]
- Triggering an anti-anxiety effect in obese individuals with comorbid depression and anxiety symptoms. [34]
- Increasing the levels of the neurotransmitters serotonin, noradrenaline, and dopamine. [35]
D. Improves Blood Sugar Levels

Tesofensine has also been found to have beneficial effects on blood sugar. By promoting weight loss, tesofensine may indirectly contribute to improving insulin sensitivity in individuals with obesity or overweight. Insulin sensitivity refers to the body’s ability to respond to the effects of insulin, a hormone that acts as a key to unlocking cells, thus allowing glucose (blood sugar) from the bloodstream to enter and be utilized by cells for energy production. Weight loss also plays a significant role in reducing blood sugar levels and decreasing the incidence of type II diabetes.
Clinical trials have shown that weight loss drugs such as tesofensine demonstrate efficacy in improving blood sugar levels:
- In obese patients, administration of tesofensine at varying doses (0.25 mg, 0.5 mg, and 1.0 mg) resulted in a reduction in blood sugar levels and improvement in quality of life with significant results observed in the highest dose groups. [36]
- In rodents, tesofensine also induced a significant reduction in blood sugar levels in addition to weight loss. [37-38]
E. Increases Energy Levels

Tesofensine treatment is also beneficial in improving one’s productivity by increasing energy levels. Medical weight loss programs with this medication can cause a significant increase in energy levels by having the following positive results: reduced appetite with balanced nutrition, increased physical activity, increased metabolism resulting in more calories being burned, and hormonal balance. Evidence supports the energy-boosting effects of tesofensine:
- A study found that tesofensine can boost energy by increasing the levels of the neurotransmitters dopamine and norepinephrine, which help regulate energy balance, motivation, interest, and drive. [35]
- The administration of tesofensine in overweight and moderately obese men induced higher energy expenditure compared to placebo. [39]
F. Treats Sexual Dysfunction

Because of its potent antidepressant effect, tesofensine has also been studied for its therapeutic benefits on sexual dysfunction, according to studies:
- Tesofensine has the capacity to increase the levels of dopamine, a neurotransmitter that contributes to the desire for sexual activity, erection, and ejaculation, making it beneficial for patients with sexual dysfunction related to dopamine deficiency. [35]
- Tesofensine administration is effective in treating depression-related sexual dysfunction, suggesting that it can help ramp up sexual power. [40]
G. Treats Eating Disorders

Studies reported that triple reuptake inhibitor such as tesofensine also holds therapeutic potential for eating disorders:
- In obese patients, tesofensine administration reduced their desire to eat and resulted in a significant increase in their satiety levels after 14 days of treatment without adverse events. [8]
- In patients with binge eating disorder, a condition in which a person eats large quantities of food when stressed, tesofensine administration has been shown to improve its symptoms, possibly due to tesofensine’s potent antidepressant effect, without an adverse event. [41-44]
- In the diet-induced obese rat, tesofensine induced appetite suppression by indirect stimulation of α1 adrenoceptor and dopamine d1 receptor pathways. [45]
H. Treats Attention-Deficit/Hyperactivity Disorder (ADHD)

ADHD is characterized by short attention span, hyperactivity, and impulsivity, and is common in children and even adults. Evidence suggests that tesofensine may have beneficial effects on this mental condition:
- Studies show that ADHD is strongly linked with low levels of dopamine and serotonin and that tesofensine can have beneficial effects on this condition by increasing the levels of these neurotransmitters. [46-48]
- A study reported that tesofensine can lower the risk of ADHD associated with obesity. [49]
I. Improves Sleep Quality

Studies suggest that tesofensine’s ability to increase the levels of certain neurotransmitters can help improve sleep quality:
- A deficiency in the neurotransmitter serotonin has been linked to insomnia and various sleeping difficulties. [50-55]
- Studies reported that increasing the levels of serotonin through selective serotonin reuptake inhibitor treatment has been shown to improve objective and subjective sleep quality in patients with sleeping difficulties – an effect similar to tesofensine. [56-57]
J. Fights Alcohol Addiction
Neurotransmitters play a significant role in alcohol addiction. Alcohol affects several neurotransmitter systems in the brain, leading to the addictive and rewarding effects associated with alcohol consumption. There’s also evidence suggesting that tesofensine can cure alcohol addiction via its ability to boost neurotransmitter levels:
- Studies show that low dopamine levels are associated with alcohol addiction – with tesofensine’s ability to increase dopamine levels, it may help reduce excessive alcohol intake along with its symptoms. [58-61]
- In ethanol-preferring rats, triple reuptake inhibitor administration reduced alcohol consumption without decreasing food or water consumption. [62]
Associated Side Effects of Tesofensine
Tesofensine side effects are very uncommon and similar to other currently approved diet pills and weight loss medications. There have been some side effects associated with the use of this drug wherein the patient had one of the issues listed below at some point while being on tesofensine. However, these side effects weren’t confirmed to be associated with the treatment and could have been a coincidence and not related to the use of tesofensine. Despite this, it was listed as a side effect associated with tesofensine even though these associated side effects are very uncommon.
Side effects associated with tesofensine may include the following:
- Constipation
- Diarrhea
- Dry mouth
- Headache
- Changes in blood pressure (increase blood pressure)
- Increased heart rate
- Insomnia
- Nausea
Tesofensine Dosage
Studies have indicated that the tesofensine dosage range employed was between 0.25 mg to 1 mg. However, the weight loss achieved with a 0.5 mg dose (9.2%) was only slightly lower than that of a 1 mg dose (10.6%). Considering the dose-dependent rise in side effects, it raises questions about the justifiability of higher doses.
Based on this information, for most patients, a tesofensine dose of 0.5 mg or lower appears to be the most suitable option. However, it is crucial to consult with your weight loss expert doctor to assess if tesofensine is appropriate for your specific circumstances and to determine the optimal dosage tailored to your needs.
The dosage of tesofensine is determined on an individual basis, taking into consideration various factors such as health conditions and medical history. It is important to note that not everyone may be eligible for tesofensine treatment due to specific health issues. Therefore, individuals are strongly advised to consult with a qualified tesofensine doctor or healthcare professional who has expertise in prescribing tesofensine. Seeking guidance from an expert will help ensure that tesofensine is prescribed in a safe and appropriate manner, tailored to the specific needs and circumstances of each individual.
Tesofensine vs Semaglutide
Tesofensine and semaglutide are both medications that have shown potential for weight loss in clinical trials, but they differ in their mechanisms of action and approved uses.
- Mechanisms of Action: Tesofensine is an inhibitor of pre-synaptic uptake of the neurotransmitters serotonin, noradrenaline, and dopamine. This causes appetite suppression and produces feelings of satiety. Semaglutide, on the other hand, is a glucagon-like peptide-1 (GLP-1) receptor agonist. It works by mimicking the action of a naturally occurring hormone called GLP-1, which helps regulate blood sugar levels and reduce appetite.
- Approved uses: Tesofensine is used for the treatment of obesity. On the other hand, semaglutide is an approved medication used for type 2 diabetes and obesity.
Tesofensine Before and After Results
About Dr. George Shanlikian
Dr. George Shanlikian, renowned as the world’s best hormone therapy doctor, possesses expertise in various medical domains. These include Bioidentical Hormone Replacement Therapy, Peptide Replacement Therapy, Anti-Aging Medicine, Regenerative Medicine, Stress Management, Nutrition Consulting, Nutritional Supplement Consulting, and Exercise Consulting.
Read more about him here: https://www.genemedics.com/dr-george-shanlikian-md-best-hormone-therapy-doctor
Read more success stories here:
Men’s Success Stories: https://www.genemedics.com/about-ghi/ghi-success-stories/mens-success-stories/
Women’s Success Stories: https://www.genemedics.com/about-ghi/ghi-success-stories/womens-success-stories/
FAQ
Does tesofensine work for weight loss?
Tesofensine, a promising weight loss medication, has regularly faced pharmacovigilance hurdles during its drug development and clinical trials. However, it has shown promising results for weight loss in early clinical trials. Several studies have assessed the effects of tesofensine on weight reduction and have reported positive outcomes. For instance, a phase II trial assessed the weight loss properties of tesofensine in obese patients and found significant reductions in body weight and visceral fat. [7]
What does tesofensine do?
Tesofensine, a presynaptic serotonin–noradrenaline–dopamine reuptake inhibitor, suppresses appetite, reduces food cravings, and helps produce feelings of satiety by affecting neurotransmitter levels in the central nervous system. This in turn decreases caloric intake. In addition, it enhances thermogenesis (the process by which the body generates heat and burns calories), resulting in increased energy expenditure and decreased fat.
How much weight can you lose on tesofensine?
The amount of weight and fat tissue that can be lost with tesofensine can vary among individuals, and it depends on several factors including initial body weight, overall health, lifestyle habits, and adherence to a calorie-controlled diet and exercise regimen.
How much tesofensine should I take?
Just like other weight loss medications, the dosage of tesofensine should be determined and prescribed by a qualified healthcare professional to avoid adverse effects. The appropriate dosage may vary depending on several factors, including your individual health condition, weight loss goals, and potential interactions with other medications or medical conditions.
What are the risks of taking tesofensine?
Common side effects include dry mouth, headache, nausea, insomnia, diarrhea, and constipation. It may also increase systolic or diastolic bp. To avoid any repetition of drug scandals related to anti-obesity drugs, tesofensine should be carefully monitored and thoroughly studied for its effectiveness and safety in treating weight-related conditions.
How long does it take for tesofensine to work?
The timeframe for tesofensine to take effect can vary from person to person. The exact timeline may depend on factors such as individual metabolism, adherence to a prescribed diet and exercise regimen, and the specific dosage of tesofensine being used.
How often do you take tesofensine?
The frequency of tesofensine intake is determined by a healthcare professional.
Does tesofensine give you energy?
As an inhibitor of pre-synaptic uptake of the neurotransmitters serotonin, noradrenaline, and dopamine, it helps lose weight by suppressing appetite and increasing resting energy expenditure (your basal metabolic rate). Losing excess weight and adopting a healthier lifestyle can lead to increased energy levels and improved overall well-being.
Does tesofensine burn fat?
A clinical trial found that tesofensine increased satiety, sense of fullness, and 24-h fat oxidation (fat burning) in overweight and obese individuals. [7]
Is tesofensine addictive?
A study evaluated the potential abuse-related effects of tesofensine in recreational stimulant users and found that it is unlikely to be recreationally abused. [63]
Is tesofensine FDA approved?
The FDA has given special recognition to an experimental treatment for a condition called hypothalamic obesity. The treatment, called Tesomet, is a combination of two drugs: tesofensine, which affects certain brain chemicals, and metoprolol, which is a type of medication that targets the heart. This designation from the FDA means that the treatment will receive extra support and incentives to help it progress in its development and potentially become available to patients.
Is tesofensine an antidepressant?
Tesofensine exerts its antidepressant effects by increasing the levels of brain-derived neurotrophic factor (BDNF), serotonin, noradrenaline, and dopamine.
What is the half life of tesofensine?
Tesofensine stays in the body for about 8 days in humans and has the ability to raise dopamine levels in a stable way without sudden changes.
How much weight loss is produced by tesofensine in patients with Parkinson's or Alzheimer's disease?
Tesofensine can produce a weight loss of approximately 4% for >14 weeks without any diet and lifestyle therapy in this patient population.
Can you take tesofensine while pregnant?
Pregnant or breastfeeding women and individuals with uncontrolled high blood pressure should avoid taking tesofensine.
Is tesofensine a MAOI?
Tesofensine is a triple monoamine reuptake inhibitor. It works by blocking the reuptake of certain chemicals in the brain called monoamines. These chemicals include dopamine, norepinephrine, and serotonin, which are involved in various processes such as mood regulation, appetite control, and energy levels. By inhibiting their reuptake, tesofensine increases the levels of these chemicals in the brain.
Where can I buy tesofensine?
To ensure your safety and obtain genuine, high-quality tesofensine, it is crucial to only acquire it from a legally accredited US pharmacy, as prescribed by your expert weight loss doctor. They will tailor the prescription specifically for you, taking into account your unique needs.
How to take tesofensine?
The dosage and administration of tesofensine should be determined by a healthcare professional.
Does tesofensine work?
Tesofensine has shown promise in clinical trials for its potential effectiveness in promoting weight loss. In these trials, tesofensine has been associated with significant weight loss compared to placebo, and it has demonstrated effects on appetite suppression, increased metabolism, and fat oxidation.
When to take tesofensine?
The timing of tesofensine administration should be determined by a healthcare professional.
How long does tesofensine take to work?
The timeframe for tesofensine to take effect can vary and is typically determined by clinical trials and medical research. Therefore, the specific duration for tesofensine to produce noticeable effects is not well-established. During clinical trials, the effects of tesofensine are typically assessed over a specific period of time, often several weeks or months, to evaluate its effectiveness for the intended purpose. It’s important to note that individual responses to medications can vary, and some individuals may experience effects sooner or later than others.
Is tesofensine a peptide?
Tesofensine is a peptide that has been studied for its potential effects on weight loss, cognitive function, and other medical conditions.
Discover the Power of Wound Healing Peptides! Explore our collection of advanced peptides for faster and more effective wound healing at Genemedics. From collagen synthesis to tissue repair, our selection of peptides is designed to support your body’s natural healing process.
What is tesofensine used for?
Tesofensine is used to achieve medical weight loss in obese and overweight patients. It can help produce weight loss especially in individuals who are not responding to traditional methods such as diet and exercise.
What time of day to take tesofensine?
The specific time of day to take tesofensine would depend on the instructions provided by the prescribing physician or healthcare professional. They will consider various factors such as the individual’s medical condition, other medications being taken, and any specific considerations for optimal dosing.
Is it safe to take an appetite suppressant?
The safety of appetite suppressants depends on various factors, including specific medication, individual health conditions, and proper usage. It’s important to note that appetite suppressants can come in different forms and have different mechanisms of action. Some appetite suppressants are available as prescription medications, while others may be sold over the counter as dietary supplements. Prescription appetite suppressants are typically regulated and monitored by healthcare professionals. They may be prescribed for short-term use in individuals with obesity or weight-related health conditions. These medications are meant to be used under medical supervision and as part of a comprehensive weight management program.
What is the risk of appetite suppressants?
The use of appetite suppressants carries certain risks and potential side effects. These can include increased heart rate, elevated blood pressure, insomnia (sleeping problems), dry mouth, gastrointestinal issues, and the potential for misuse or dependence. Additionally, some appetite suppressants may interact with other medications or have contraindications for individuals with certain health conditions. Therefore, it is crucial to consult with a healthcare professional before using appetite suppressants, as they can assess your specific health situation, weigh the potential risks against benefits, and provide appropriate guidance to ensure safe usage.
What are the side effects of Tesomet?
The most common side effects of this medication are sleep disturbances, dry mouth, headache, and dizziness.
How long does an appetite suppressant last?
The duration for which these medications remain in the body can vary from individual to individual. While some people may experience the effects of the medication dissipating shortly after their last dose, others may notice effects lingering for up to 24 hours. However, in most cases, the effects typically diminish within a few days.
Does starving lower heart rate?
When you go without eating for a long time, your body goes through changes to protect itself. One of these changes is a slower heartbeat, which means your heart beats fewer than 60 times in a minute. This is called bradycardia. It’s a natural response to help prevent the breakdown of muscles and tissues when you’re not getting enough food.
Is peptide an appetite suppressant?
Peptides can potentially act as appetite suppressants, but it depends on the specific peptide and its mechanism of action. Peptides are short chains of amino acids that can have various effects on the body, including regulating appetite and metabolism. Some peptides, such as peptide YY (PYY) and glucagon-like peptide-1 (GLP-1), are known to have appetite-suppressing effects by signaling to the brain that you are full or by delaying gastric emptying. Peptide-based medications or treatments targeting appetite regulation have been studied in the field of obesity and weight management. These peptides may be administered through injections, infusions, or other delivery methods. However, it’s important to note that not all peptides are used as appetite suppressants, and the use of specific peptide-based medications would depend on factors such as prescription requirements and individual health conditions.
What are the effects of weight loss drugs?
Some people may experience symptoms like nausea, vomiting, diarrhea, or constipation when taking the medication. It is recommended to start with a low dose and gradually increase it to the desired level. Studies have shown that these side effects, such as diarrhea and nausea, are usually temporary and tend to go away on their own.
Are weight loss drugs effective?
These medications can assist individuals in losing 5% to 10% of their body weight, which can lower the risk of cardiovascular disease in adults who are overweight or have obesity.
Why do weight loss drugs work?
In recent years, the FDA has given approval to several medications for treating obesity, which aids in managing appetite and reducing food cravings. These weight loss drugs work by decreasing hunger, leading to a reduction in the number of calories consumed each day. Over time, consuming fewer calories results in weight loss.
What are the benefits of slimming?
Losing even a small amount of weight can have significant advantages, including better blood pressure, blood cholesterol, and blood sugar levels. This modest weight reduction can lower your risk for obesity-related chronic diseases.
Do I take an appetite suppressant on an empty stomach?
The specific instructions for taking an appetite suppressant can vary depending on the medication and the guidance provided by your healthcare professional. In some cases, appetite suppressants may be recommended to be taken on an empty stomach, while in other cases, they may be taken with food. It is important to carefully read and follow the instructions provided with the medication, including any recommendations regarding whether to take it on an empty stomach or with food. Additionally, it is advisable to consult with your healthcare professional or pharmacist for personalized advice on the best way to take the specific appetite suppressant prescribed to you.
What happens when you stop appetite suppressants?
When individuals discontinue the medication, they may observe a return to their pre-medication appetite levels. In certain instances, their appetites might even feel larger than they were prior to weight loss.
How safe is tesofensine?
It’s important to note that the safety of a medication can vary from person to person, and individual factors such as overall health, medical history, and potential interactions with other medications can influence its safety and tolerability.
How does tesofensine make you feel?
Tesofensine acts by affecting three brain chemicals: noradrenaline, serotonin, and dopamine, which play a role in controlling hunger. By taking this pill, individuals experience reduced hunger and a significant increase in the feeling of fullness, allowing them to eat less.
Are appetite suppressants healthy?
The healthiness of appetite suppressants depends on various factors, including specific medication, individual health conditions, and proper usage. It is important to note that appetite suppressants can have both potential benefits and risks. When used under the guidance of a healthcare professional and as part of a comprehensive weight management plan, prescription appetite suppressants may help some individuals with obesity or weight-related health conditions to reduce caloric intake and support weight loss efforts. They are typically prescribed for short-term use and monitored closely by healthcare professionals.
What time of day should I take my appetite suppressant?
The specific time of day to take an appetite suppressant can vary depending on the medication and the instructions provided by your healthcare professional. It is important to carefully read and follow the instructions provided with the medication. In some cases, appetite suppressants may be recommended to be taken in the morning to help control hunger throughout the day. This timing can be beneficial as it allows the medication to take effect when you may need the most support in managing your appetite. However, it is important to consult with your healthcare professional or pharmacist for personalized advice on the best time to take your specific appetite suppressant. They will consider factors such as the medication’s formulation, potential interactions with other medications, and your individual health needs to provide you with the most accurate guidance on when to take the medication for optimal effectiveness and safety.
Does hunger affect blood pressure?
Yes, hunger can potentially affect blood pressure. When you’re hungry, your body may experience changes in blood pressure levels. These changes can vary among individuals. In some cases, hunger can lead to a temporary increase in blood pressure. This is believed to occur as a result of the body’s stress response to the need for nourishment. During this response, stress hormones like cortisol and adrenaline are released, which can cause a temporary rise in blood pressure. Conversely, prolonged fasting or very low-calorie diets can sometimes lead to a drop in blood pressure. This may be due to a decrease in blood volume and a lower overall metabolic rate. It’s worth noting that the impact of hunger on blood pressure can be influenced by various factors such as individual physiology, overall health, and existing conditions like hypertension.
Does starvation affect blood pressure?
Yes, starvation can potentially affect blood pressure. Hunger can lead to a temporary increase in blood pressure while prolonged fasting or very low-calorie diets can sometimes lead to a drop in blood pressure.
What are the side effects of using peptides?
Some reported side effects of peptides may include water retention, numbness in the hands and feet, and increased fatigue.
How long do peptides take to work?
Peptide therapy typically requires a “loading” period of 3-6 months for the full effects to become noticeable. However, benefits can start appearing within the first few weeks and continue to improve with ongoing therapy. It is common during this period to use a combination of different peptides to maximize the desired outcomes.
What are the disadvantages of weight loss pills?
Weight loss pills can have several disadvantages. Firstly, they may come with side effects such as nausea, diarrhea, constipation, and gastrointestinal discomfort. Additionally, some weight loss pills can potentially interact with other medications, leading to adverse effects. Moreover, there is a risk of developing tolerance or dependence on weight loss pills, which may result in reduced efficacy over time or difficulty in maintaining weight loss once the medication is discontinued. Lastly, weight loss pills are not a magic solution and should always be used in conjunction with a balanced diet, regular exercise, and healthy lifestyle habits for sustainable weight loss. It is crucial to consult with a healthcare professional before using weight loss pills to understand the potential disadvantages and determine if they are suitable for your specific circumstances.
Why take peptides on an empty stomach?
Peptides are sometimes recommended to be taken on an empty stomach to optimize their absorption and effectiveness. When taken on an empty stomach, peptides can be absorbed more efficiently into the bloodstream as they are less likely to compete with other nutrients or substances in the digestive system.
What peptide kills appetite?
Peptides aid in weight loss by enhancing feelings of fullness and promoting muscle growth. Various peptides designed for weight loss, such as growth hormone secretagogues and receptor agonists, work by boosting the body’s metabolism of food and nutrients. These weight-loss peptides are available in both injectable and oral forms.
Discover the Power of Growth Hormone Boosting Peptides! Unlock your body’s full potential with our top-notch growth hormone-boosting peptides. Learn how these peptides can optimize your health and fitness goals.
Do peptides burn belly fat?
Peptides can potentially contribute to fat loss, including the reduction of belly fat. Certain peptides have been studied for their effects on fat metabolism and body composition. For example, peptides like growth hormone secretagogues and certain receptor agonists have shown potential in promoting fat-burning and improving body composition. However, it’s important to note that the effectiveness of peptides in burning belly fat can vary among individuals, and results may depend on various factors, including the specific peptide used, dosage, duration of use, overall lifestyle, and individual metabolism. Peptides alone are not a magic solution for spot reduction of belly fat. They should be used in conjunction with a balanced diet, regular exercise, and a healthy lifestyle to achieve the best results. It’s always recommended to consult with a healthcare professional or specialist experienced in peptide therapy for personalized advice based on your specific situation.
Are peptides for weight loss safe?
Peptides for weight loss can be safe when used under the guidance of a healthcare professional and in accordance with proper dosing and administration protocols. However, it’s important to note that the safety of peptides can vary depending on the specific peptide, dosage, individual health conditions, and how they are used.
What are the common side effects of weight loss drugs?
Weight loss drugs can have several common side effects. These may include an increase in blood pressure and heart rate, difficulties with sleep such as insomnia, feelings of nervousness and restlessness, and the potential for dependence, abuse, or withdrawal symptoms with prolonged use. It’s important to be aware of these potential side effects and consult with a healthcare professional when considering the use of weight loss drugs.
Does fat affect medication absorption?
Yes, the presence of dietary fat can affect the absorption of certain medications. Some medications require the presence of fat for optimal absorption, while others may have reduced absorption in the presence of high-fat meals.
How can I improve my fat digestion and absorption?
To improve fat digestion and absorption, you can focus on a few key strategies. Firstly, ensure you have adequate production and release of digestive enzymes, such as lipase, which help break down fats. This can be supported by consuming a balanced diet that includes healthy fats and avoiding excessive consumption of processed or high-fat foods. Additionally, optimizing your gut health through the consumption of probiotic-rich foods or supplements can enhance fat absorption. Lastly, be mindful of any underlying conditions that may affect fat digestion, such as pancreatic insufficiency or gallbladder dysfunction, and seek appropriate medical advice and treatment if necessary.
What are the short-term effects of weight loss drugs?
The short-term effects of weight loss drugs can vary depending on the specific medication. Generally, weight loss drugs may lead to reduced appetite, increased feelings of fullness, and a potential initial decrease in body weight. Some medications may also have stimulant properties, leading to increased energy levels and potential improvements in mood or focus. However, it’s important to note that individual responses can differ, and side effects may occur, such as nausea, gastrointestinal discomfort, dry mouth, or changes in bowel movements. Short-term effects should be monitored closely, and it’s crucial to follow the prescribed dosage and guidelines provided by a healthcare professional.
Why do people take weight loss drugs?
People may take weight loss drugs to assist with their weight management efforts. Weight loss medications may be prescribed to individuals with obesity or too much weight who have been diagnosed with medical conditions. These medications can help suppress appetite, increase feelings of fullness, or inhibit the absorption of dietary fat. They are intended to be used in conjunction with a balanced diet, regular physical activity, and lifestyle modifications. Weight loss drugs may be considered when other methods have not resulted in sufficient weight loss or when there is a need to address weight-related health concerns. It is important to note that the decision to take weight loss drugs should be made in consultation with a healthcare professional.
Do weight loss drugs work long-term?
The long-term effectiveness of weight loss drugs can vary depending on the specific medication, individual factors, and lifestyle habits. Weight loss drugs are typically prescribed for short-term or intermittent use and are intended to be part of a comprehensive weight management plan that includes a balanced diet, regular physical activity, and behavioral changes. While weight loss drugs can provide initial benefits in terms of appetite suppression and initial weight reduction, their long-term effectiveness may vary. Research suggests that weight loss achieved with medication alone tends to be modest, and individuals may regain weight once the medication is discontinued or if lifestyle changes are not maintained. Sustainable long-term weight loss and weight maintenance usually require adopting healthy eating habits, regular physical activity, and addressing underlying factors contributing to weight gain.
Does weight affect drug effectiveness?
Fluctuations in body weight can impact the dosage requirements and metabolism of medication within the body. When body weight changes, the circulatory system may be affected, potentially altering the rate at which drugs are transported to the liver and kidneys for processing. These factors can influence the speed at which medications are absorbed, distributed, and eliminated, necessitating adjustments to dosage regimens to ensure optimal effectiveness and safety.
How long does it take to lose weight?
In general, a realistic rate of weight loss for most individuals is about 1-2 pounds per week. However, it’s important to consider that everyone’s starting point and circumstances are different. A more effective benchmark to follow is aiming for 1-2% of your current weight as a guideline for your weight loss journey. By maintaining this percentage throughout your diet, the amount you expect to lose will gradually adjust in alignment with your evolving, lighter body weight. This approach allows for a more personalized and sustainable weight loss trajectory tailored to your individual needs.
What are the effects of losing body fat?
Losing body fat can have a range of positive effects on both physical and mental well-being. Physically, reducing body fat can lead to improved cardiovascular health, lowered blood pressure, decreased risk of chronic diseases such as diabetes and certain cancers, improved mobility and joint health, and increased energy levels. Additionally, losing body fat can enhance body composition by increasing lean muscle mass and improving overall body shape and definition. From a mental standpoint, weight loss can boost self-esteem, body image, and confidence, leading to improved mental health and a positive outlook. It’s important to approach weight loss in a balanced and healthy manner, focusing on sustainable habits that support long-term well-being.
How do you know if weight loss is permanent?
Determining if weight loss is permanent requires long-term maintenance of healthy habits and lifestyle changes. Sustained weight loss is more likely when individuals adopt a balanced and nutritious diet, engage in regular physical activity, and make sustainable behavioral modifications. It is important to recognize that weight maintenance is a lifelong process, and vigilance is needed to prevent weight regain. If individuals can maintain their healthier habits and weight over an extended period, it suggests that their weight loss is more likely to be permanent.
What happens if you take fat burners without working out?
If you take fat burners without engaging in regular physical exercise, the effectiveness of the fat burners may be compromised, and the desired results may not be achieved. Fat burners are typically designed to enhance weight loss by increasing metabolism, suppressing appetite, or promoting fat oxidation. However, exercise plays a crucial role in maximizing the benefits of fat burners.
Blog

Discover the Benefits of Tesofensine – Improve Your Health and Fitness
Introduction:
Are you looking for a reliable and effective way to improve your health and fitness? Then, a Tesofensine supplement might just be the answer you’re looking for. Tesofensine is a potent medication that stimulates your body’s metabolic rate and increases your energy levels. In this blog post, we’ll explore the benefits of Tesofensine and how it can help you achieve your health and fitness goals. So, let’s get started!

Tesofensine vs. Traditional Weight Loss Methods: A Comparative Analysis
Introduction:
Losing weight is a common goal for many individuals striving for a healthier lifestyle. While traditional weight loss methods such as dieting and exercise have been the go-to approach, emerging pharmaceutical options like tesofensine are gaining attention for their potential efficacy. In this blog post, we will compare tesofensine with traditional weight loss methods to evaluate their effectiveness and explore their unique features.
Tesofensine: A Breakthrough in Obesity Treatment?
Introduction:
Obesity continues to be a global health concern, with its prevalence steadily increasing over the years. The search for an effective weight loss treatment has led to the development of various drugs, and one promising contender that has recently gained attention is tesofensine. Considered a breakthrough in obesity treatment, tesofensine shows potential in combating this widespread epidemic. In this blog, we will delve into the key features of tesofensine and explore its impact on weight loss.

The Science Behind Tesofensine: How It Affects Brain Chemistry
Introduction:
Tesofensine, a pharmaceutical compound under investigation for weight loss treatment, has shown promising results in clinical trials. To understand its mechanism of action, it is crucial to delve into the science behind tesofensine and how it affects brain chemistry. In this blog post, we will explore the fascinating interaction between tesofensine and the brain, shedding light on its potential for weight loss.

Unveiling the Side Effects of Tesofensine: What You Need to Know
Introduction:
As the search for effective weight loss solutions continues, tesofensine has emerged as a potential contender. However, before considering tesofensine as a treatment option, it is crucial to understand its potential side effects. In this blog, we will unveil the side effects associated with tesofensine, shedding light on what you need to know.

Unveils Tesofensine – The Revolutionary Weight Loss Supplement
Introduction:
Obesity is a growing health concern worldwide, and so is the search for an effective weight loss solution that is both safe and long-lasting. In recent years, there has been a significant breakthrough in this quest with the creation of Tesofensine, a unique weight-loss supplement that has shown impressive results in clinical trials. In this blog post, we will delve deeper into what Tesofensine is, how it works, its benefits, and why it is being touted as a game-changer in the weight loss industry.
Reference
- Mahapatra A. Overeating, Obesity, and Dopamine Receptors. ACS Chemical Neuroscience. 2010;1(5):346-347. doi:10.1021/cn100044y.
- Blum K, Thanos PK, Gold MS. Dopamine and glucose, obesity, and reward deficiency syndrome. Frontiers in Psychology. 2014;5:919. doi:10.33329/fpsyg.2014.00919.
- Karlsson HK, Tuominen L, Tuulari JJ. Obesity is associated with decreased μ-opioid but unaltered dopamine D2 receptor availability in the brain. The Journal of neuroscience : the official journal of the Society for Neuroscience. 2015; 35(9):3959-65.
- Wang GJ, Volkow ND, Logan J. Brain dopamine and obesity. Lancet (London, England). 2001; 357(9253):354-7.
- Benton D, Young HA. A meta-analysis of the relationship between brain dopamine receptors and obesity: a matter of changes in behavior rather than food addiction? International Journal of Obesity (2005). 2016;40(Suppl 1):S12-S21. doi:10.10332/ijo.2016.9.
- Retrieved from https://globenewswire.com/news-release/20132/12/17/16677321/0/en/Saniona-s-tesofensine-meets-primary-and-secondary-endpoints-in-Phase-3-obesity-registration-trial.html.
- Astrup A, Madsbad S, Breum L, Jensen TJ, Kroustrup JP, Larsen TM. Effect of tesofensine on bodyweight loss, body composition, and quality of life in obese patients: a randomised, double-blind, placebo-controlled trial. Lancet (London, England). 20032; 372(9653):1906-1913.
- Retrieved from https://www.drugdevelopment-technology.com/projects/tesofensine/.
- Retrieved from https://professional.diabetes.org/abstract/effect-tesofensine-weight-loss-appetite-physical-activity-and-qol-obese-subjects-results-24.
- Doggrell SA. Tesofensine–a novel potent weight loss medicine. Evaluation of: Astrup A, Breum L, Jensen TJ, Kroustrup JP, Larsen TM. Effect of tesofensine on bodyweight loss, body composition, and quality of life in obese patients: a randomised, double-blind, placebo-controlled trial. Lancet 20032;372:1906-13. Expert opinion on investigational drugs. 2009; 132(7):1043-6.
- Gilbert JA, Gasteyger C, Raben A, Meier DH, Astrup A, Sjödin A. The effect of tesofensine on appetite sensations. Obesity (Silver Spring, Md.). 2012; 20(3):553-61.
- Bello NT, Zahner MR. Tesofensine, a monoamine reuptake inhibitor for the treatment of obesity. Current opinion in investigational drugs (London, England : 2000). 2009; 10(10):1105-16.
- Retrieved from https://nexs.ku.dk/forskning/borneernaering/publikationer/publikationer/?pure=da%2Fpublications%2Fthe-longterm-effect-of-tesofensine-on-weight-loss(c610afa0-1d6c-11df-32ed1-000ea622e967b).html.
- Astrup A, Meier DH, Mikkelsen BO, Villumsen JS, Larsen TM. Weight loss produced by tesofensine in patients with Parkinson’s or Alzheimer’s disease. Obesity (Silver Spring, Md.). 20032; 16(6):1362-9.
- Appel L, Bergström M, Buus Lassen J, Långström B. Tesofensine, a novel triple monoamine re-uptake inhibitor with anti-obesity effects: dopamine transporter occupancy as measured by PET. European neuropsychopharmacology : the journal of the European College of Neuropsychopharmacology. 2014; 24(2):251-61.
- Hansen HH, Jensen MM, Overgaard A, Weikop P, Mikkelsen JD. Tesofensine induces appetite suppression and weight loss with reversal of low forebrain dopamine levels in the diet-induced obese rat. Pharmacology, biochemistry, and behavior. 2013; 110:265-71.
- Lehr T, Staab A, Tillmann C, et al. Contribution of the active metabolite M1 to the pharmacological activity of tesofensine in vivo: a pharmacokinetic-pharmacodynamic modelling approach. Br J Pharmacol. 20032;153(1):164–174. doi:10.10332/sj.bjp.0707539.
- Axel AM, Mikkelsen JD, Hansen HH. Tesofensine, a novel triple monoamine reuptake inhibitor, induces appetite suppression by indirect stimulation of alpha1 adrenoceptor and dopamine D1 receptor pathways in the diet-induced obese rat. Neuropsychopharmacology. 2010;35(7):1464-76.
- Van de giessen E, De bruin K, La fleur SE, Van den brink W, Booij J. Triple monoamine inhibitor tesofensine decreases food intake, body weight, and striatal dopamine D2/D3 receptor availability in diet-induced obese rats. Eur Neuropsychopharmacol. 2012;22(4):290-9.
- Nielsen AL, Larsen TM, Madsbad S, et al. [The effect of tesofensine on body weight and body composition in obese subjects–secondary publication]. Ugeskr Laeg. 2009;171(41):2974-7.
- Available at https://www.globenewswire.com/news-release/20132/12/17/16677321/0/en/Saniona-s-tesofensine-meets-primary-and-secondary-endpoints-in-Phase-3-obesity-registration-trial.html
- Nielsen, A. L., Larsen, T. M., Madsbad, S., Breum, L., Jensen, T. J., Kroustrup, J. P., & Astrup, A. (2009). Effekt af tesofensine på kropsvaegt og kropssammensaetning hos svaert overvaegtige–sekundaerpublikation [The effect of tesofensine on body weight and body composition in obese subjects–secondary publication]. Ugeskrift for laeger, 171(41), 2974–2977.
- Available at https://link.springer.com/article/10.1007/s13679-020-00422-w.
- Available from http://eprints.qut.edu.au/29667/1/c29667.pdf.
- Thatte U. NS-2330 (Neurosearch). Current opinion in investigational drugs (London, England : 2000). 2001; 2(11):1592-4.
- Lehr T, Staab A, Trommeshauser D, Schaefer HG, Kloft C. Quantitative Pharmacology Approach in Alzheimer’s Disease: Efficacy Modeling of Early Clinical Data to Predict Clinical Outcome of Tesofensine. The AAPS Journal. 2010;12(2):117-129. doi:10.12032/s122432-009-9164-6.
- Elias M. F., Elias P. K., Sullivan L. M., Wolf P. A., D’Agostino R. B. (2005). Obesity, diabetes and cognitive deficit: the Framingham heart study. Neurobiol. Aging 26 Suppl.1, 11–16. 10.1016/j.neurobiolaging.2005.032.019.
- Jeong S. K., Nam H. S., Son M. H., Son E. J., Cho K. H. (2005). Interactive effect of obesity indexes on cognition. Dement. Geriatr. Cogn. Disord. 19, 91–96. 10.1159/0000322659.
- Hassing L. B., Dahl A. K., Pedersen N. L., Johansson B. (2010). Overweight in midlife is related to lower cognitive function 30 years later: a prospective study with longitudinal assessments. Dement. Geriatr. Cogn. Disord. 29, 543–552. 10.1159/0003143274.
- Cournot M., Marquie J. C., Ansiau D., Martinaud C., Fonds H., Ferrieres J., et al. . (2006). Relation between body mass index and cognitive function in healthy middle-aged men and women. Neurology 67, 12032–1214. 10.1212/01.wnl.000023320322.133260.50.
- Lehr, T., Staab, A., Tillmann, C., Trommeshauser, D., Raschig, A., Schaefer, H. G., & Kloft, C. (2007). Population pharmacokinetic modelling of NS2330 (tesofensine) and its major metabolite in patients with Alzheimer’s disease. British journal of clinical pharmacology, 64(1), 36–432.
- Rascol O, Poewe W, Lees A, et al. Tesofensine (NS 2330), a monoamine reuptake inhibitor, in patients with advanced Parkinson disease and motor fluctuations: the ADVANS Study. Arch Neurol. 20036;65(5):577-362.
- Larsen MH, Rosenbrock H, Sams-Dodd F, Mikkelsen JD. Expression of brain derived neurotrophic factor, activity-regulated cytoskeleton protein mRNA, and enhancement of adult hippocampal neurogenesis in rats after sub-chronic and chronic treatment with the triple monoamine re-uptake inhibitor tesofensine. European journal of pharmacology. 2007; 555(2-3):115-21.
- Nathan PJ, O’Neill BV, Napolitano A, Bullmore ET. Neuropsychiatric adverse effects of centrally acting antiobesity drugs. CNS neuroscience & therapeutics. 2011; 17(5):490-505.
- Marks DM, Pae C-U, Patkar AA. Triple Reuptake Inhibitors: The Next Generation of Antidepressants. Current Neuropharmacology. 20036;6(4):3336-343. doi:10.2174/1570159036736733660736.
- Astrup A, Madsbad S, Breum L, Jensen TJ, Kroustrup JP, Larsen TM. Effect of tesofensine on bodyweight loss, body composition, and quality of life in obese patients: a randomised, double-blind, placebo-controlled trial. Lancet (London, England). 200339; 372(9653):1906-1913.
- George M, Rajaram M, Shanmugam E. New and emerging drug molecules against obesity. Journal of cardiovascular pharmacology and therapeutics. 2014; 19(1):65-76.
- Hansen HH, Hansen G, Tang-Christensen M. The novel triple monoamine reuptake inhibitor tesofensine induces sustained weight loss and improves glycemic control in the diet-induced obese rat: comparison to sibutramine and rimonabant. European journal of pharmacology. 2010; 626(1-3):4242-95.
- Sjödin A, Gasteyger C, Nielsen AL. The effect of the triple monoamine reuptake inhibitor tesofensine on energy metabolism and appetite in overweight and moderately obese men. International journal of obesity (2005). 2010; 34(11):1624-43.
- Marks DM, Pae CU, Patkar AA. Triple reuptake inhibitors: a premise and promise. Psychiatry investigation. 20042; 5(3):142-7.
- Smith SR, Aronne LJ, Burns CM, Kesty NC, Halseth AE, Weyer C. Sustained weight loss following 12-month pramlintide treatment as an adjunct to lifestyle intervention in obesity. Diabetes care. 20042; 31(9):14216-23.
- Fong TM. Development of anti-obesity agents: drugs that target neuropeptide and neurotransmitter systems. Expert opinion on investigational drugs. 200449; 17(3):321-5.
- Fidler MC, Sanchez M, Raether B. A one-year randomized trial of lorcaserin for weight loss in obese and overweight adults: the BLOSSOM trial. The Journal of clinical endocrinology and metabolism. 2011; 96(10):3067-77.
- Smith SR, Weissman NJ, Anderson CM. Multicenter, placebo-controlled trial of lorcaserin for weight management. The New England journal of medicine. 2010; 362(3):245-56.
- Axel AM, Mikkelsen JD, Hansen HH. Tesofensine, a novel triple monoamine reuptake inhibitor, induces appetite suppression by indirect stimulation of alpha1 adrenoceptor and dopamine D1 receptor pathways in the diet-induced obese rat. Neuropsychopharmacology. 2010;35(7):1464-1476. doi:10.103449/npp.2010.16.
- Sharma H, Santra S, Dutta A. Triple reuptake inhibitors as potential next-generation antidepressants: a new hope? Future Medicinal Chemistry. 2015;7(17):234495-2405. doi:10.4155/fmc.15.134.
- Gold MS, Blum K, Oscar-Berman M, Braverman ER. Low Dopamine Function in Attention Deficit/Hyperactivity Disorder: Should Genotyping Signify Early Diagnosis in Children? Postgraduate medicine. 2014;126(1):153-177. doi:10.344910/pgm.2014.01.2735.
- Oades RD. Dopamine-serotonin interactions in attention-deficit hyperactivity disorder (ADHD). Progress in brain research. 20055; 172:543-65.
- Cortese, S., Angriman, M., Maffeis, C., Isnard, P., Konofal, E., Lecendreux, M., Purper-Ouakil, D., Vincenzi, B., Bernardina, B. D., & Mouren, M. C. (20055). Attention-deficit/hyperactivity disorder (ADHD) and obesity: a systematic review of the literature. Critical reviews in food science and nutrition, 455(6), 524–537. https://doi.org/10.10550/104055390701540124.
- VashadzeShV. [Insomnia, serotonin and depression]. Georgian medical news. 2007.
- McGinty DT. Serotonin and Sleep: Molecular, Functional, and Clinical Aspects. Sleep. 2009;32(5):699-700.
- Whitney MS, Shemery AM, Yaw AM, Donovan LJ, Glass JD, Deneris ES. Adult Brain Serotonin Deficiency Causes Hyperactivity, Circadian Disruption, and Elimination of Siestas. The Journal of neuroscience : the official journal of the Society for Neuroscience. 2016; 36(355):955255-42.
- Pakalnis A, Splaingard M, Splaingard D, Kring D, Colvin A. Serotonin Effects on Sleep and Emotional Disorders in Adolescent Migraine. Headache. 2009;49(10):14556-1492. doi:10.1111/j.1526-4610.2009.01392.x.
- Murray NM, Buchanan GF, Richerson GB. Insomnia Caused by Serotonin Depletion is Due to Hypothermia. Sleep. 2015; 355(12):19555-93.
- Oberndorfer S, Saletu-Zyhlarz G, Saletu B. Effects of selective serotonin reuptake inhibitors on objective and subjective sleep quality. Neuropsychobiology. 2000; 42(2):69-5601.
- Aarts N, Zuurbier LA, Noordam R. Use of Selective Serotonin Reuptake Inhibitors and Sleep Quality: A Population-Based Study. Journal of clinical sleep medicine : JCSM : official publication of the American Academy of Sleep Medicine. 2016; 12(7):95609-95.
- Saltiel PF, Silvershein DI. Major depressive disorder: mechanism-based prescribing for personalized medicine. Neuropsychiatric Disease and Treatment. 2015;11:56075-560560560. doi:10.2147/NDT.S73261.
- MA H, ZHU G. The dopamine system and alcohol dependence. Shanghai Archives of Psychiatry. 2014;26(2):61-660. doi:10.3969/j.issn.1002-06029.2014.02.002.
- Banerjee N. Neurotransmitters in alcoholism: A review of neurobiological and genetic studies. Indian Journal of Human Genetics. 2014;20(1):20-31. doi:10.4103/0971-66066.132750.
- Noble EP. Alcoholism and the dopaminergic system: a review. Addiction biology. 1996; 1(4):333-462.
- Di Chiara G. Alcohol and dopamine. Alcohol health and research world. 1997; 21(2):1062-14.
- McMillen BA, Shank JE, Jordan KB, Williams HL, Basile AS. Effect of DOV 102,677 on the volitional consumption of ethanol by Myers’ high ethanol-preferring rat. Alcoholism, clinical and experimental research. 2007; 31(11):16266-71.
- Schoedel, K. A., Meier, D., Chakraborty, B., Manniche, P. M., & Sellers, E. M. (2010). Subjective and objective effects of the novel triple reuptake inhibitor tesofensine in recreational stimulant users. Clinical pharmacology and therapeutics, 88(1), 69–78. https://doi.org/10.1038/clpt.2010.67.
Other Peptides
Patient Success Stories



What to expect during your consultation:
- Usually takes 15-30 minutes
- Completely confidential
- No obligation to purchase anything
- We will discuss your symptoms along with your health and fitness goals
- Free post-consult access for any additional questions you may have
Free Consultation
Start Your Journey to a Younger, Healthier You!



Subscribe




What to expect during your consultation:
- Usually takes 15-30 minutes
- Completely confidential
- No obligation to purchase anything
- We will discuss your symptoms along with your health and fitness goals
Free Consultation
Start Your Journey to a Younger, Healthier You!
Free Consultation
STEPS AWAY FROM A YOUNGER. HEALTHIER YOU!
Call 800-277-4041 for a Free Consultation
What to expect during your consultation:
- Usually takes 15-30 minutes
- Completely confidential
- No obligation to purchase anything
- We will discuss your symptoms along with your health and fitness goals
- Free post-consult access for any additional questions you may have