
Potential Benefits of Ibutamoren (MK 677)
MK 677 offers a variety of benefits, including improving lean muscle mass, promoting fat loss, maintaining a healthy skeletal frame, enhancing sleep quality, and boosting cognitive function. Additionally, it accelerates wound healing, supports heart health, strengthens the immune system, enhances sexual function and drive, improves blood sugar levels, and positively influences cholesterol profiles.
- Improves lean muscle mass and promotes fat loss [3-26]
- Maintains a healthy skeletal frame [27-56]
- Improves sleep quality [57-81]
- Improves cognitive function [82-136]
- Accelerates wound healing and tissue regeneration [137-150]
- Maintains a healthy heart [151-202]
- Strengthens the immune system [203-240]
- Improves sex drive and sexual function [241-273]
- Improves blood sugar levels [273-308]
- Improves cholesterol profile [309-332]
Key Takeaways of Ibutamoren (MK 677)
- Ibutamoren, commonly known as MK-677, is a growth hormone secretagogue that stimulates the pituitary gland to release more growth hormone and insulin-like growth factor 1 (IGF-1).
- MK-677 benefits include improved muscle mass, fat loss, healthy bones, improved cognitive function, enhanced wound healing and tissue regeneration, healthy heart, strong immune system, improved sex drive and sexual function, improved blood sugar levels, and improved cholesterol profile.
- MK-677 has several potential advantages over anabolic steroids, as it promotes muscle growth, increases bone mineral density, and aids in recovery without the adverse side effects associated with traditional steroids. Unlike traditional anabolic steroids, MK-677 is considered safer and does not suppress natural hormone production, making it a promising option for muscle growth without major side effects.
- The usual recommended dosage range for MK-677 is between 10-25 mg per day, typically administered once daily. However, some individuals may prefer dividing the dosage into two or three smaller administrations. To ensure safety and effectiveness, it is advisable to commence with a lower dose and incrementally adjust until finding the optimal dosage that suits your needs.
- When considering purchasing MK-677, it is crucial to ensure that you obtain it from a legally accredited US pharmacy. It is recommended to do so only under the guidance and prescription of a qualified weight loss doctor who can tailor the dosage and treatment plan specifically for your individual needs and health condition. Buying MK-677 from reputable sources and following your doctor’s instructions will help ensure its quality, safety, and effectiveness in supporting your weight loss journey.
What is Ibutamoren (MK 677)?
MK-677, also known as MK 677, ibutamoren, or ibutamoren mesylate, belongs to a group called growth hormone secretagogues. They are substances that boost growth hormone production. MK-677 can also increase the production of insulin-like growth factor 1 (IGF-1), a hormone similar in molecular structure and function to insulin. The ability of MK-677 to boost the levels of GH and IGF-1 is associated with a wide array of health benefits.
Discover the transformative power of Growth Hormone Boosting Peptides for enhanced muscle growth and recovery. Explore our cutting-edge peptides collection to unlock your body’s full potential. Elevate your fitness journey with science-backed solutions to optimize your growth hormone levels today!
How Ibutamoren (MK 677) Works
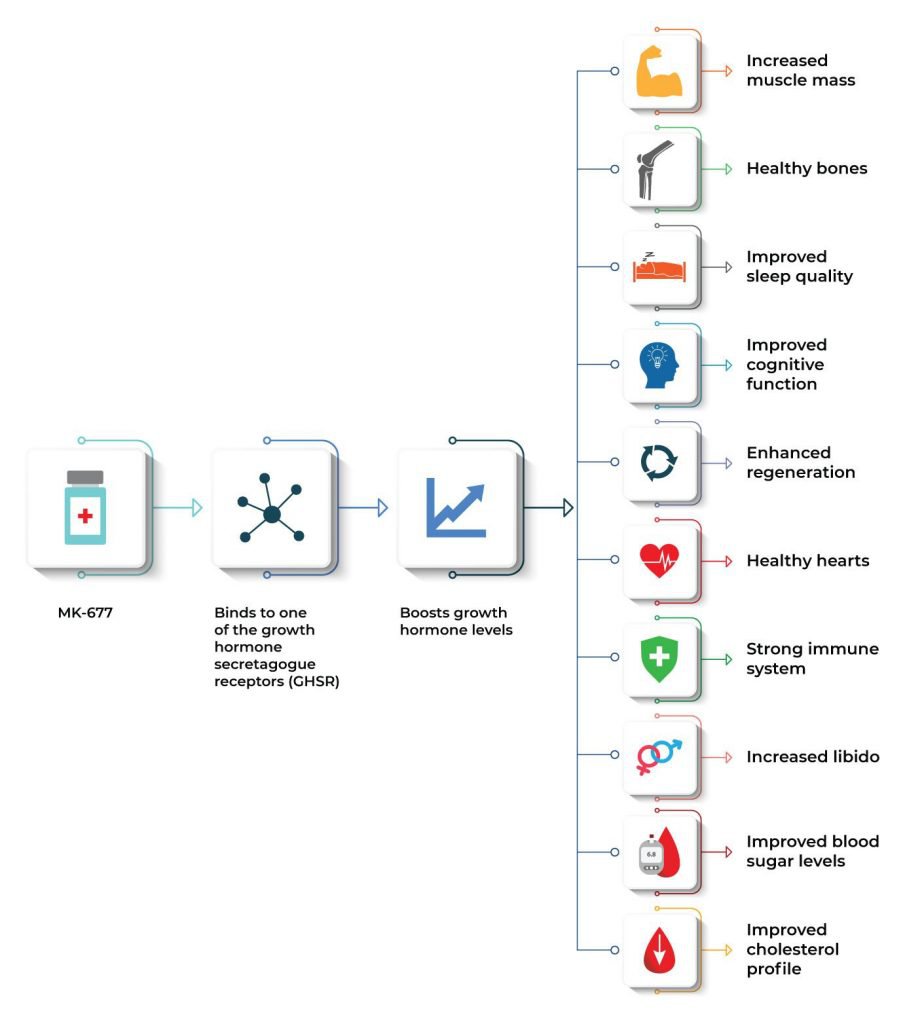
The exact mechanism by which Ibutamoren (MK 677) exerts these effects is by mimicking the action of the hunger hormone ghrelin and binding to one of the growth hormone secretagogue receptors (GHSR) in the brain. [1] This in turn boosts growth hormone (GH) levels. Interestingly, GHSR is located in certain regions of the brain that regulate appetite, mood, pleasure, and cognitive function. [2] Because of this, researchers believe that MK-677 can have beneficial effects on these functions.
In addition, MK-677 is also classified as a selective androgen receptor modulator (SARM), a class of therapeutic compounds similar in function to anabolic agents, but with lesser side effects. This makes MK-677 a safe and effective form of GH and IGF-1 replacement therapy.
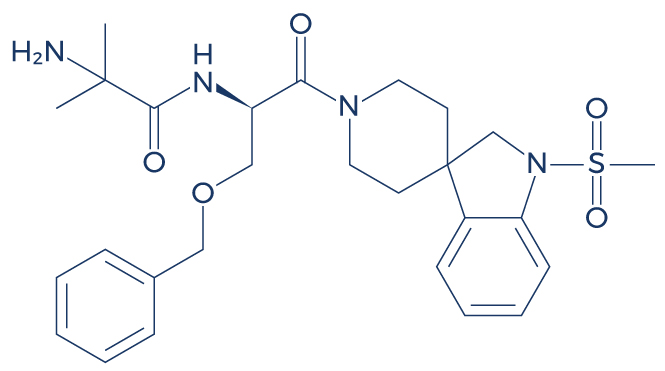
Chemical Structure of Ibutamoren (MK 677)
Research on Ibutamoren (MK 677)
A Improves Lean Muscle Mass and Promotes Fat Loss

Ibutamoren (MK 677) can produce a peak GH response by stimulating the release of growth hormone from the pituitary gland, leading to a sudden increase in circulating GH levels in the bloodstream. This peak response is observed shortly after ingestion and contributes to the various benefits associated with MK-677, such as enhanced muscle growth, fat loss, and improved body composition.
MK-677 is frequently used as an anabolic substance, which means that it can produce physical benefits such as increased muscle mass and strength as well as fat loss. Studies show that this powerful compound can help improve body composition and prevent muscle wasting related to old age and other medical conditions:
- In obese males, oral treatment with MK-677 increased fat-free mass by boosting basal metabolic rate (BMR), the rate at which the body uses energy while at rest. [3]
- Several high-quality studies showed that higher GH levels were strongly linked with increased muscle mass and strength in the elderly, suggesting that MK-677 supplementation may have positive effects. [4-13]
- Several lines of evidence also suggested that higher IGF-1 levels were associated with increased muscle mass and strength in the older population. [14-22]
- In patients with muscle wasting, MK-677 reversed diet-induced nitrogen wasting with higher tolerability and without clinically significant adverse experiences. Neither the serum cortisol response nor the PRL response showed a significant increase after 7 days of MK-677 dosing when compared with 7 days of placebo. There was no significant difference in IGF binding protein-2 observed between the MK-677 and placebo treatments. [23]
- In patients recovering from hip fracture, MK-677 treatment improved gait speed and stair climbing power, which is suggestive of improved muscle function. [24]
- In healthy older adults, 12 months of MK-677 treatment significantly increased fat-free mass without any adverse side effects. [25]
- In GH-deficient adults, MK-677 administration improved body composition by increasing IGF-1 levels. [26]
Discover the power of Peptides for Weight Loss – Explore more options now! Take the first step towards your weight loss goals today.
B. Maintains a Healthy Skeletal Frame

MK-677 belongs to a class of drugs known as growth hormone secretagogues, which work by stimulating the pituitary gland to produce and release more growth hormones. This enhanced production of growth hormone, along with the increased release of insulin-like growth factor 1 (IGF-1), plays a crucial role in promoting various physiological processes. One notable benefit of MK-677 is its ability to increase bone mineral density, which can be particularly beneficial for individuals looking to enhance bone health and strength.
Increased growth hormone and IGF-1 improve bone health by stimulating the cells responsible for bone formation, leading to higher bone density and strength. These hormones promote the synthesis of new bone tissue and help maintain bone mass, reducing the risk of fractures and promoting overall bone health. Clinical studies support MK-677’s ability to increase bone density and improve overall bone health:
- In healthy obese males, MK-677 treatment for 2 weeks improved bone turnover (total volume of bone formed and broken down). [27]
- In elderly adults (65 years or older), oral MK-677 treatment daily for 2 weeks improved bone building by increasing osteocalcin, a marker of bone turnover. [28]
- In postmenopausal women with osteoporosis, MK-677 treatment for 12 months improved bone mineral density in the femoral neck. [29]
- In patients with hip fracture (no more than 18 days post-fracture), daily treatment with MK-677 for 6 months resulted in greater improvement in three of four lower extremity functional performance measures and in the ability to live independently compared with placebo treatment. [30]
- A study reported that increased GH can stimulate the mobilization of endothelial progenitor cells (EPCs) from the bone marrow to the sites of injury, suggesting that MK-677 can help repair damaged bones. [31]
- A study found that MK-677 can improve bone health by increasing the activity of osteoblasts (bone cells). [32]
- By increasing GH levels, MK-677 can significantly lower the risk of osteoporosis, fractures, and other bone disorders. [33-45]
- By boosting IGF-1 levels, MK-677 can also help lower the prevalence of various bone disorders. [46-56]
C. Improves Sleep Quality

Enhanced release of growth hormone induced by MK-677 promotes good sleep because growth hormone plays a crucial role in regulating the sleep-wake cycle. It helps improve the quality of sleep by increasing the time spent in deep, restorative sleep stages. Additionally, growth hormone aids in muscle repair and recovery during sleep, leading to a more restful and rejuvenating sleep experience. As a result, individuals taking MK-677 often experience better sleep patterns and overall sleep quality.
The aging population is highly at risk for sleep problems and disorders that can significantly affect the quality of life. Whether it is age-related or caused by a certain medical condition, Ibutamoren (MK 677) supplementation may help improve sleep quality and quantity according to numerous clinical trials:
- In both younger and elderly subjects, MK-677 treatment for 14 days improved sleep quality by increasing rapid eye movement (REM) sleep duration by 50%. [57]
- In healthy older adults, oral administration of MK-677 (25 mg) once daily improved the Pittsburgh Sleep Quality Index, a measure of sleep. [58]
- In normal men, the administration of growth hormone secretagogue increases slow-wave sleep (SWS), which is often referred to as deep sleep. [59]
- In young healthy men, intravenous injections of growth hormone secretagogue during sleep consistently stimulated slow-wave sleep, suggesting that MK-677 may help improve sleep quality. [60]
- In healthy young adults, growth hormone secretagogue administration increases stage 2 sleep. [61]
- Higher GH levels are strongly associated with improved deep sleep stage, indicating that MK-677 supplementation may have positive effects on sleep. [62-67]
- Higher IGF-1 levels are also linked with better sleep, suggesting that MK-677 supplementation may have beneficial effects. [68-78]
- Studies on rats showed that growth hormone secretagogue administration activated sleep-regulatory neurons in the brain. [79]
- In obese patients, growth hormone secretagogue administration improved stage 2 sleep by reversing GH deficiency. [80-81]
D. Improves Cognitive Function
Doctors usually prescribe Ibutamoren (MK 677) for patients suffering from cognitive impairment because of its nootropic benefits. Nootropics are drugs, supplements, and other substances that have the ability to improve certain aspects of cognitive function such as learning, memory, creativity, and motivation. Several high-quality clinical studies support the beneficial effects of MK-677 on various cognitive functions and overall brain health:
- By increasing REM sleep duration and sleep quality, MK-677 can help improve cognitive function. [82-83]
- In older adults, the administration of growth hormone secretagogues improved short-term memory and active problem-solving skills, suggesting that MK-677 may also exert beneficial effects on cognitive function. [84]
- In adults with mild cognitive impairment and healthy older adults, 20 weeks of growth hormone secretagogue administration improved executive function and verbal memory. [85]
- MK-677 has also been found to improve various aspects of cognitive function by increasing IGF-1 levels. [86-90]
- With increased IGF-1 levels, the body activates intracellular pathways involved in the protection of nerve cells in the brain. [91-108]
- MK-677 also protects brain cells against programmed cell death (apoptosis) by increasing ghrelin levels, which in turn prevents cognitive decline. [109-114]
- MK-677 improves cognitive function and prevents age-related cognitive decline by increasing the levels of GH. [115-129]
- The administration of growth hormone secretagogues improves cognitive function by increasing the levels of brain chemicals such as gamma-Aminobutyric acid and N-acetyl-aspartyl-glutamate. [130]
- In healthy older adults, the administration of growth hormone secretagogues helped combat age-related cognitive decline and Alzheimer’s disease. [131]
- In rat models of Alzheimer’s disease, MK-677 administration reduced the formation of abnormal proteins known as amyloid beta (causative agent of AD). [132]
- SARMs such as MK-677 stimulate the growth and development of brain tissues, enhance communication of nerve cells (neurons), and promote brain cell survival. [133-136]
E. Accelerates Wound Healing and Tissue Regeneration
Growth hormone secretagogues such as Ibutamoren (MK 677) have the ability to accelerate the repair of damaged tissues caused by physical trauma or sports-related injuries. There is compelling evidence supporting the regenerative properties of MK-677:
- By boosting GH levels, MK-677 accelerates the migration of cells into the injured or damaged tissues, thus speeding up the wound healing process. [137-139]
- MK-677 can also speed up the wound healing process by increasing skin thickness. [140]
- MK-677 speeds up wound healing by increasing wound collagen content, granulation tissue, and wound tensile strength. [141-143]
- MK-677 increases IGF-1 levels, which in turn stimulates wound healing by increasing cell proliferation and collagen synthesis. [144-147]
- In mice, SARMs administration prevented damage to the central nervous system and improved regeneration by reducing inflammatory substances. [148]
- In rats, growth hormone secretagogue administration improved functional recovery after various injuries by stimulating the formation of new neuronal cells. [149]
- In mice, the administration of growth hormone secretagogue enhanced the healing of skin wounds resulting from trauma, surgery, or disease. [150]
Discover the power of advanced Wound Healing Peptides to accelerate recovery and promote tissue regeneration. Explore our range of cutting-edge products designed to optimize the wound healing process and enhance your body’s natural healing mechanisms. Take the first step towards faster and more effective wound healing today.
F. Maintains a Healthy Heart
Heart disease ranks among the top in terms of mortality worldwide. Interestingly, Ibutamoren (MK 677) possesses potent cardioprotective properties that can help reduce the prevalence of heart disease and the rate of deaths associated with this condition. Recent research suggests that MK-677 and other growth hormone secretagogues can help preserve heart function through various important mechanisms:
- In obese patients, MK-677 treatment improved heart health by reducing low-density lipoprotein (bad cholesterol). [151]
- By increasing ghrelin levels, MK-677 prevents programmed cell death of cardiomyocytes (heart cells). [152-154]
- By increasing GH levels, MK-677 significantly reduces the risk of heart disease and related deaths. [155-164]
- By increasing IGF-1 levels, MK-677 also reduces the risk of heart disease and related deaths. [165-180]
- MK-677 and other growth hormone secretagogues protect against myocardial infarction by activating signaling pathways responsible for self-renewal and survival of cardiac cells. [181-188]
- MK-677 also induces cardiac repair after myocardial infarction. [189-191]
- In animal models, MK-677 and other growth hormone secretagogues stimulated the self-renewal of cardiac stem cells and promoted their survival. [192-195]
- In mice, growth hormone secretagogue administration restored the electrical activity of the heart. [196]
- In rats, growth hormone secretagogue administration protected against heart damage induced by reduced oxygen. [197-201]
- In mice, growth hormone secretagogue administration stimulated the formation of new cardiac tissues. [202]
G. Strengthens the Immune System
Ibutamoren (MK 677) and other growth hormone secretagogues have the ability to enhance the immune response. Research suggests that they play a role in the regulation of immune function through the following important mechanisms:
- In humans, growth hormone secretagogues modulate the immune function through stimulation of the GH/insulin-like growth factor-1 (IGF-I) axis. [203-206]
- In the elderly, both short- and long-term growth hormone secretagogue administration increased the numbers of lymphocytes, monocytes, B-cells, and T-cells. [207]
- Growth hormone secretagogues can also modulate the immune function through brain mechanisms involved in sleep regulation. [208]
- By increasing GH levels, MK-677 helps regulate T cell development, cytokine production, B cell development, antibody production, neutrophil adhesion, monocyte migration, and anti-apoptotic action. [209-210]
- By increasing GH levels, MK-677 also significantly lowers the risk of various diseases related to a compromised immune system. [211-222]
- By increasing IGF-1 levels, MK-677 also significantly lowers the risk of autoimmune diseases and other immune system-related disorders. [223-237]
- By boosting ghrelin levels, MK-677 strengthens the immune system by lowering inflammation. [238]
- In animal models, the administration of growth hormone secretagogues increased the numbers of CD2+ αβ T-cells, CD25+CD4+ cells, and CD4+CD45R+ cells in the immune system. [239-240]
H. Improves Sex Drive and Sexual Function
The ability of Ibutamoren (MK 677) to positively influence the levels of vital hormones such as GH and IGF-1 can help improve sex drive and sexual function. There is strong scientific evidence supporting the beneficial effects of MK-677 and other growth hormone secretagogues on the sexual health of both men and women:
- MK-677 indirectly improves sexual function by increasing GH and IGF-1 levels, which in turn boosts the levels of nitric oxide, a naturally occurring substance that induces harder and longer penile erections. [241-249]
- Another mechanism by which MK-677 improves libido is by increasing testosterone and estrogen levels, which are hormones that regulate sexual desire and sexual function. [250-251]
- By boosting ghrelin levels, MK-677 also helps improve sexual function. [252-255]
- A growing body of clinical evidence suggests that growth hormone deficiency is strongly linked with low libido and erectile dysfunction, suggesting that boosting GH levels through MK-677 supplementation may help ramp up sexual power. [256-264]
- Studies also showed that IGF-1 deficiency is strongly linked with low libido and erectile dysfunction, suggesting that MK-677 may have beneficial effects on sex drive and sexual function. [265-271]
- In healthy postmenopausal women, growth hormone secretagogue supplementation improved libido without any adverse side effects. [272]
- In age-advanced men and women, 4 months of growth hormone secretagogue supplementation improved general well-being and libido. [273]
I. Improves Blood Sugar Levels
Ibutamoren (MK 677) and other growth hormone secretagogues have potent anti-diabetic properties. There is compelling evidence supporting the ability of MK-677 to bring down elevated levels of blood sugar in diabetic patients and animal models:
- In diabetic patients, MK-677 administration improved the body’s response to the effects of insulin, which in turn lowers blood sugar levels. [274]
- In diabetic patients, MK-677 administration significantly reduced blood sugar levels by increasing GH secretion. [275]
- MK-677 boosts IGF-1 levels, which in turn lowers blood sugar levels. [276-287]
- MK-677 also boosts GH levels, which results in a significant reduction in blood sugar levels. [288-301]
- In diabetic rats, growth hormone secretagogue administration enhanced insulin secretion, which in turn lowered blood sugar levels. [302-303]
- In diabetic rats, pre-treatment with growth hormone secretagogue improved insulin secretion and insulin reserve. [304-308]
J. Improves Cholesterol Profile
Chronic elevation in cholesterol levels significantly increases one’s risk of stroke, heart disease, hypertension, and other deadly diseases. According to studies, one can greatly reduce their risk for these debilitating medical conditions by reducing cholesterol levels through Ibutamoren (MK 677) supplementation:
- In obese patients, MK-677 treatment reduced the levels of low-density lipoprotein, which is known as bad cholesterol. [309]
- In older men and women, growth hormone secretagogue administration significantly reduced total cholesterol levels. [310]
- In older adults, growth hormone secretagogue administration reduced low-density lipoprotein levels without any adverse side effects. [311]
- By increasing GH levels, MK-677 can help bring down elevated cholesterol levels. [312-321]
- By boosting IGF-1 levels, MK-677 can also help reduce low-density lipoprotein levels and increase high-density lipoprotein (good cholesterol). [322-331]
- In rats with abnormal cholesterol profiles, growth hormone secretagogue administration reduced cholesterol levels. [332]
Unlocking the Power of MK-677: How Nitrogen Balance Boosts Muscle Growth and Fat Loss
One of the significant benefits of MK-677 is that it promotes an increased nitrogen balance in the body. This refers to the balance between the amount of nitrogen taken in through dietary protein and the amount of nitrogen excreted from the body.
During a cutting phase, when someone is in a caloric deficit, there is an increased risk of muscle catabolism, where the body breaks down muscle tissue for energy. This process can hinder muscle growth and lead to a loss of muscle mass. However, MK-677’s ability to enhance nitrogen balance helps offset this diet-induced catabolism by preserving more muscle tissue.
When you have a positive nitrogen balance (more nitrogen retained than excreted), it signals an environment that promotes muscle growth and repair. By maintaining a positive nitrogen balance during cutting, MK-677 allows individuals to continue building muscle while simultaneously losing fat. This is considered a remarkable feat because typically, losing fat and gaining muscle are two separate and often challenging processes. However, with MK-677’s influence on nitrogen balance, it becomes more achievable to attain these goals simultaneously.
It is essential to note that individual responses to MK-677 can vary, and the effectiveness of this process depends on various factors, including diet, exercise, and overall health. If considering MK-677 or any other supplement, it’s crucial to consult with a healthcare professional to ensure it is safe and appropriate for individual circumstances.
Muscle Rebuilding: Unveiling the Synergistic Power of MK-677, Ghrelin, and Human Growth Hormone for Optimal Gains
MK-677, also known as Ibutamoren, stimulates the release of growth hormone (GH) and interacts with ghrelin receptors, which are the same receptors that the hunger hormone ghrelin binds to. By activating these receptors, MK-677 can mimic the effects of ghrelin in certain tissues. When ghrelin is released, it stimulates appetite and increases food consumption, which can lead to a surplus of nutrients available for muscle growth. Additionally, ghrelin has been found to stimulate the release of growth hormone.
The increase in growth hormone levels brought about by MK-677 and ghrelin can contribute to muscle rebuilding and growth as well as other key benefits through several mechanisms:
- Protein Synthesis: Growth hormone plays a crucial role in promoting protein synthesis in muscles. It enhances the uptake of amino acids into muscle cells, leading to increased protein production and muscle repair.
- Muscle Preservation: MK-677 can help preserve muscle mass during periods of caloric deficit or catabolic states. This is particularly beneficial during cutting phases or when the body is under stress, as it aids in preventing muscle breakdown.
- IGF-1 Production: Growth hormone stimulates the liver to produce insulin-like growth factor 1 (IGF-1). IGF-1 is an anabolic hormone that plays a key role in muscle growth and repair, promoting the proliferation of muscle cells.
- Enhanced Recovery: By promoting deeper and more restful sleep, MK-677 supports better recovery. Adequate rest and recovery are essential for muscle rebuilding and overall athletic performance.
- Energy Metabolism: By enhancing growth hormone and IGF-1, MK-677 encourages the utilization of nutrients like glucose and amino acids for energy production, leading to improved muscle function and performance during physical activities.
It’s important to note that while MK-677 can provide benefits for muscle rebuilding, its effects may vary from person to person, and it should be used responsibly and under proper medical supervision. Additionally, individual responses to MK-677 can be influenced by factors such as diet, exercise regimen, and overall health.
Unlocking the Power of MK-677 Bulking Stack: Amplifying Muscle Growth through Enhanced Nitrogen Balance and Blood Glucose Utilization
The MK-677 bulking stack has gained immense popularity among bodybuilders and fitness enthusiasts for its remarkable ability to unlock the true potential of muscle growth. At the heart of its effectiveness lies the unique combination of enhanced nitrogen balance and blood glucose utilization. MK-677, a growth hormone secretagogue, stimulates the production and release of growth hormone, leading to an increase in insulin-like growth factor 1 (IGF-1). This growth-promoting environment fosters heightened protein synthesis and cellular regeneration, creating the perfect foundation for substantial muscle gains.
One of the key mechanisms through which MK-677 supports muscle growth is by influencing nitrogen balance. Nitrogen, an essential component of proteins, is crucial for building and repairing muscle tissues. MK-677 enhances nitrogen retention in muscle cells, facilitating a positive nitrogen balance, where the body retains more nitrogen than it excretes. This anabolic state allows for increased muscle protein synthesis, promoting faster recovery from workouts and ultimately leading to more significant muscle growth.
Moreover, the bulking stack’s impact on blood glucose utilization plays a pivotal role in fueling muscle development. MK-677 has been shown to increase blood glucose levels, resulting in higher availability of energy for the muscles. As a result, muscle cells are better equipped to uptake glucose, converting it into glycogen, the primary energy source for intense workouts. The surplus energy enables athletes to train harder and longer, breaking through plateaus and experiencing accelerated muscle hypertrophy (growth).
In conclusion, the MK-677 bulking stack harnesses the power of enhanced nitrogen balance and blood glucose utilization to revolutionize muscle growth. By promoting a highly anabolic environment and providing ample energy for intense training, MK-677 paves the way for substantial gains in lean muscle mass. When combined with a well-structured training program and proper nutrition, this stack becomes a potent tool in the arsenal of those seeking to take their physique and performance to new heights.
Optimizing Muscle Growth: The Ideal MK-677 Cycle Length for Maximum Results
The typical MK-677 cycle length ranges from 8 to 12 weeks. However, some individuals may choose to extend it up to 16 weeks, but this should be approached with caution due to potential side effects and diminishing returns on muscle growth beyond a certain point. It is essential to follow the recommended dosage guidelines and cycle length to ensure safety and maximize the benefits of MK-677 without compromising long-term health.
After completing a cycle, it is advisable to take a break and allow the body to recover before considering another cycle. Always consult a healthcare professional or qualified expert before starting any supplement or cycle to ensure it aligns with individual health goals and needs.
Ibutamoren (MK 677): Unlocking the Advantages of a Safer Growth Hormone Secretagogue over Anabolic Steroids
MK-677, also known as Ibutamoren, offers several key advantages as a growth hormone secretagogue that distinguish it from traditional anabolic steroids. These advantages make it a popular choice among bodybuilders and athletes seeking enhanced performance and muscle growth without some of the drawbacks associated with steroids:
- Enhanced Muscle Growth: MK-677 stimulates the production of growth hormone, leading to increased muscle mass and strength. Unlike anabolic steroids, it promotes lean muscle gains without excess fat and unwanted side effects such as water retention and bloating.
- Fat Loss: By boosting growth hormone levels, MK-677 helps facilitate fat loss and improves body composition. It promotes the utilization of stored fat as an energy source, making it an ideal option for those aiming to achieve a leaner physique.
- Safety Profile: Unlike anabolic steroids, MK-677 does not suppress natural testosterone production, reducing the risk of hormone imbalances and post-cycle therapy. It is also non-toxic to the liver, which is a common concern with some oral steroids.
- No Estrogenic Effects: Estrogenic side effects, such as gynecomastia (development of breast tissue in males), are not observed with MK-677. This is a significant advantage over certain anabolic steroids that can lead to estrogen-related complications.
- Joint and Tissue Repair: MK-677 aids in collagen synthesis, benefiting joint and ligament health. This makes it valuable for athletes and bodybuilders who undergo rigorous training and may experience joint stress.
- Oral Administration: MK-677 is taken orally in the form of a pill, eliminating the need for injections common with some anabolic steroids. This ease of administration makes it a more convenient option for many users.
MK 677 vs Other Growth Hormone Boosting Peptides
A. MK 677 vs CJC-1295
MK-677 and CJC-1295 are both peptides that have been shown to increase growth hormone (GH) levels. However, they have different mechanisms of action and may have different effects on the body.
MK-677 is a non-peptide GH secretagogue, which means that it works by mimicking the action of the hormone ghrelin. Ghrelin is a hormone that is produced by the stomach and stimulates the release of GH from the pituitary gland. MK-677 has been shown to increase GH levels by up to 300%.
CJC-1295 is a synthetic growth hormone releasing hormone (GHRH). GHRH is a hormone that is produced by the hypothalamus and stimulates the pituitary gland to release GH. CJC-1295 has been shown to increase GH levels by up to 200%.
In addition to increasing GH levels, MK-677 has also been shown to increase insulin-like growth factor 1 (IGF-1) levels. IGF-1 is a hormone that is produced by the liver and acts on many tissues in the body, including muscle, bone, and fat. IGF-1 is responsible for many of the anabolic effects of GH, such as increased muscle growth and strength.
CJC-1295 does not appear to increase IGF-1 levels to the same extent as MK-677. However, CJC-1295 has been shown to have a longer half-life than MK-677, meaning that it stays in the body for longer and provides a more sustained release of GH.
Overall, MK-677 and CJC-1295 are both effective at increasing GH levels. However, MK-677 appears to have more anabolic effects than CJC-1295, while CJC-1295 has a longer half-life. The best peptide for you will depend on your individual goals and preferences.
B. MK 677 vs Ipamorelin
MK-677 and Ipamorelin are both growth hormone secretagogues (GHS), which means they stimulate the pituitary gland to release growth hormone (GH). However, they have different mechanisms of action and may have different effects on the body.
MK-677 is a non-peptide GHS, which means it is a small molecule that can be taken orally. It works by binding to the ghrelin receptor, which is a receptor that is also activated by the hormone ghrelin. Ghrelin is a hormone that is produced by the stomach and is involved in appetite regulation and growth hormone release. MK-677 has been shown to increase GH levels by up to 300%.
Ipamorelin is a peptide GHS, which means it is a chain of amino acids. It works by binding to the growth hormone secretagogue receptor (GHSR), which is a receptor that is also activated by the hormone GHRH. GHRH is a hormone that is produced by the hypothalamus and is involved in the release of GH from the pituitary gland. Ipamorelin has been shown to increase GH levels by up to 200%.
In addition to increasing GH levels, MK-677 has also been shown to increase insulin-like growth factor 1 (IGF-1) levels. IGF-1 is a hormone that is produced by the liver and acts on many tissues in the body, including muscle, bone, and fat. IGF-1 is responsible for many of the anabolic effects of GH, such as increased muscle growth and strength.
Ipamorelin does not appear to increase IGF-1 levels to the same extent as MK-677. However, Ipamorelin has been shown to have a longer half-life than MK-677, meaning that it stays in the body for longer and provides a more sustained release of GH.
Overall, MK-677 and Ipamorelin are both effective at increasing GH levels. However, MK-677 appears to have more anabolic effects than Ipamorelin, while Ipamorelin has a longer half-life. The best peptide for you will depend on your individual goals and preferences.
C. MK 677 vs Tesamorelin
MK-677 and Tesamorelin are both peptides that have been shown to increase growth hormone (GH) levels. However, they have different mechanisms of action and may have different effects on the body.
MK-677 is a non-peptide GH secretagogue, which means that it works by mimicking the action of the hormone ghrelin. Ghrelin is a hormone that is produced by the stomach and stimulates the release of GH from the pituitary gland. MK-677 has been shown to increase GH levels by up to 300%.
Tesamorelin is a synthetic growth hormone releasing hormone (GHRH). GHRH is a hormone that is produced by the hypothalamus and stimulates the pituitary gland to release GH. Tesamorelin has been shown to increase GH levels by up to 200%.
In addition to increasing GH levels, MK-677 has also been shown to increase insulin-like growth factor 1 (IGF-1) levels. IGF-1 is a hormone that is produced by the liver and acts on many tissues in the body, including muscle, bone, and fat. IGF-1 is responsible for many of the anabolic effects of GH, such as increased muscle growth and strength.
Tesamorelin does not appear to increase IGF-1 levels to the same extent as MK-677. However, Tesamorelin has been shown to have a longer half-life than MK-677, meaning that it stays in the body for longer and provides a more sustained release of GH.
Overall, MK-677 and Tesamorelin are both effective at increasing GH levels. However, MK-677 appears to have more anabolic effects than Tesamorelin, while Tesamorelin has a longer half-life. The best peptide for you will depend on your individual goals and preferences.
D. MK 677 vs Sermorelin
MK-677 and Sermorelin are both peptides that have been shown to increase growth hormone (GH) levels. However, they have different mechanisms of action and may have different effects on the body.
MK-677 is a non-peptide GH secretagogue, which means that it works by mimicking the action of the hormone ghrelin. Ghrelin is a hormone that is produced by the stomach and stimulates the release of GH from the pituitary gland. MK-677 has been shown to increase GH levels by up to 300%.
Sermorelin is a synthetic growth hormone releasing hormone (GHRH). GHRH is a hormone that is produced by the hypothalamus and stimulates the pituitary gland to release GH. Sermorelin has been shown to increase GH levels by up to 200%.
In addition to increasing GH levels, MK-677 has also been shown to increase insulin-like growth factor 1 (IGF-1) levels. IGF-1 is a hormone that is produced by the liver and acts on many tissues in the body, including muscle, bone and fat. IGF-1 is responsible for many of the anabolic effects of GH, such as increased muscle growth and strength.
Sermorelin does not appear to increase IGF-1 levels to the same extent as MK-677. However, Sermorelin has been shown to have a longer half-life than MK-677, meaning that it stays in the body for longer and provides a more sustained release of GH.
Overall, MK-677 and Sermorelin are both effective at increasing GH levels. However, MK-677 appears to have more anabolic effects than Sermorelin, while Sermorelin has a longer half-life. The best peptide for you will depend on your individual goals and preferences.
Ibutamoren (MK 677) Dosage
The typical dosage of MK-677 is 10-25 mg per day. It is typically taken once per day, but some people may choose to split the dose into two or three smaller doses. It is important to start with a low dose and gradually increase it to find the best dosage for you.
There is no one-size-fits-all answer to the question of how much MK-677 you should take. The best way to determine the right dosage for you is to talk to your doctor or a qualified healthcare professional. They can help you assess your individual needs and recommend a dosage that is safe and effective for you.
Here are some things to keep in mind when determining your MK-677 dosage:
- Your weight: The dosage of MK-677 may need to be adjusted based on your weight.
- Your age: Older adults may need a lower dosage than younger adults.
- Your health status: If you have any health conditions, such as diabetes or high blood pressure, you may need to start with a lower dosage and increase it more slowly.
- Your goals: If you are taking MK-677 for muscle growth, you may need a higher dosage than if you are taking it for other purposes, such as increasing your appetite or improving your sleep.
MK-677 Before and After Results
About Dr. George Shanlikian
Dr. George Shanlikian, renowned as the world’s best hormone therapy doctor, possesses expertise in various medical domains. These include Bio-Identical Hormone Replacement Therapy, Peptide Replacement Therapy, Anti-Aging Medicine, Regenerative Medicine, Stress Management, Nutrition Consulting, Nutritional Supplement Consulting, and Exercise Consulting.
Read more about him here: https://www.genemedics.com/dr-george-shanlikian-md-best-hormone-therapy-doctor
Read more success stories here:
Men’s Success Stories: https://www.genemedics.com/about-ghi/ghi-success-stories/mens-success-stories/
Women’s Success Stories: https://www.genemedics.com/about-ghi/ghi-success-stories/womens-success-stories/
Ibutamoren (MK 677) Side Effects
MK-677 side effects are very uncommon. There have been some side effects associated with the use of this drug wherein the patient had one of the issues listed below at some point while being on MK-677. However, these side effects weren’t confirmed to be associated with the treatment and could have been a coincidence and not related to the use of MK-677. Despite this, it was listed as a side effect associated with MK-677 even though these associated side effects are very uncommon.
Side effects associated with MK-677 may include the following:
- Headaches
- Increased appetite
- Increased blood sugar levels
- Increased insulin levels
- Increased levels of the stress hormone cortisol
- Sleepiness
- Mild lower extremity edema
- Muscle pain
FAQ
How long does it take to see the effects of MK-677?
The time it takes to see the effects of MK-677 can vary from person to person. Some individuals may start noticing certain effects, such as improved sleep patterns, within the first two weeks of taking MK-677. However, for other benefits like increased muscle mass, fat loss, increased bone density, or body weight gain due to muscle growth, it may take several weeks or even months to become noticeable.
What is the most effective way to take MK-677?
The time it takes to see the effects of MK-677 can vary from person to person. Some individuals may start noticing certain effects, such as improved sleep pattens, within the first two weeks of taking MK-677. However, for other benefits like increased muscle mass or fat loss, it may take several weeks or even months to become noticeable.
MK-677 works by stimulating the release of growth hormones, which can lead to various positive effects on the body. These effects may occur gradually over time as the body responds to the increased growth hormone levels. Patience is important when taking MK-677, as the full benefits may take some time to manifest.
What to know when taking MK-677?
When taking MK-677, there are several important things to know:
- Dosage: Take MK-677 as directed by the product label or your healthcare provider. Typically, it is taken once daily, usually at night.
- Patience: MK-677’s effects may take time to become noticeable. Be patient and consistent with its use to see potential benefits.
- Potential Side Effects: Like any supplement, MK-677 may have side effects. Common ones include increased appetite and blood sugar levels. Talk to your doctor if you experience any unusual symptoms.
- Interactions: Inform your healthcare provider about any other medications or supplements you are taking to check for potential interactions with MK-677.
- Not a Magic Pill: MK-677 can be helpful for some, but it is not a magic solution for fitness or health goals. It works best when combined with a healthy diet and exercise routine.
- Consult a Healthcare Provider: Before starting MK-677 or any new supplement, consult with your healthcare provider to ensure it is safe and appropriate for your specific health needs.
- Individual Responses Vary: Results from MK-677 can differ from person to person. What works for one may not work the same for another.
How much muscle can I gain with MK-677?
The amount of muscle gain you can achieve with MK-677 can vary from person to person. MK-677 is not a muscle-building steroid, but it may help support muscle growth indirectly by increasing growth hormone levels in the body. The extent of muscle gain depends on several factors, including:
- Diet: Consuming enough protein and calories to support muscle growth is essential.
- Exercise: Regular strength training exercises can promote muscle development.
- Individual Response: People may respond differently to MK-677, and genetics play a role in muscle-building potential.
- Duration of Use: The length of time you use MK-677 may influence the results.
Does MK-677 affect sleep?
Yes, MK-677 can affect sleep in some individuals. One of the potential benefits of MK-677 is improved sleep quality. Many people who take MK-677 report experiencing better and deeper sleep, which can contribute to better overall rest and recovery.
Is MK-677 good for cutting?
MK-677 is not specifically designed as a cutting supplement, but it may have some benefits that could be helpful during a cutting phase. Cutting is a term used in bodybuilding and fitness to describe a phase where individuals aim to reduce body fat while maintaining muscle mass.
MK-677, although more commonly known for its bulking properties, offers a unique advantage during cutting phases due to its ability to boost nitrogen balance. This means it effectively counteracts diet-induced protein breakdown and nitrogen loss, preserving valuable muscle mass. In simpler terms, when combined with the right diet, this stack aids in fat shredding without sacrificing muscle, with a focus on preventing diet-induced protein catabolism.
MK-677 may indirectly support a cutting phase in the following ways:
- Muscle Preservation: MK-677 may help preserve lean muscle, which is important during cutting to avoid excessive muscle loss.
- Improved Recovery: Better sleep and potential benefits on muscle recovery could be helpful during intense workouts.
- Increased Metabolism: Some users report increased food intake with MK-677, which could potentially aid in meeting caloric needs during a cutting diet.
Does MK-677 need PCT?
No, MK-677 does not typically require Post Cycle Therapy (PCT). Post Cycle Therapy (PCT) is a process used by some people who have taken anabolic steroids or other performance-enhancing substances. In simple terms, it’s like a “recovery plan” for the body after using these substances. When someone takes steroids, their body’s natural hormone production gets disrupted, and PCT helps the body get back to normal.
PCT usually involves taking different medications or supplements to support the body in restoring its natural hormone balance. The goal of PCT is to minimize side effects, maintain the gains made during steroid use, and help the body recover safely and efficiently.
MK-677 is not a traditional anabolic steroid or hormone. It is a growth hormone secretagogue that stimulates the release of growth hormone and insulin-like growth factor 1 (IGF-1) in the body. Unlike anabolic steroids, MK-677 does not directly interfere with the body’s natural growth hormone production itself, and it does not typically require Post Cycle Therapy (PCT).
Does MK-677 make you heal faster?
MK-677 may potentially help with faster healing indirectly. MK-677 is a growth hormone secretagogue, which means it can increase the body’s production of growth hormones. Growth hormone is known to play a role in the process of tissue repair and regeneration.
By increasing growth hormone levels, MK-677 may support the body’s natural healing processes and contribute to faster recovery from injuries or workouts. It could aid in repairing damaged tissues and promoting overall healing.
Does MK-677 burn fat?
MK-677 is not a fat-burning supplement itself, but it may indirectly support fat loss in some individuals. MK-677 is a growth hormone secretagogue, which means it increases the body’s production of growth hormones. Growth hormone plays a role in metabolism and can help the body break down fats for energy.
By boosting growth hormone levels, MK-677 may assist in maintaining lean muscle during weight loss efforts. More muscle can lead to a higher metabolic rate, which can help burn calories and potentially support fat loss.
Does MK-677 speed up recovery?
Yes, MK-677 may potentially help speed up recovery after workouts or physical activities. MK-677 is a growth hormone secretagogue, which means it increases the body’s production of growth hormones. Growth hormone plays a crucial role in the recovery and repair of tissues and muscles after exercise or injury.
By increasing growth hormone levels, MK-677 may aid in faster recovery from intense workouts, reduce muscle soreness, and enhance overall healing processes. This can allow individuals to bounce back quicker and be ready for their next training session.
How does MK-677 make you feel?
MK-677 can make people feel differently based on their individual responses. Some people may experience positive effects, while others may not notice any significant changes.
The most commonly reported effects of MK-677 include:
- Improved Sleep: Some individuals may experience better sleep quality and feel more rested.
- Increased Appetite: MK-677 can sometimes lead to a greater appetite, which can be beneficial for those looking to gain weight or increase muscle mass.
- Enhanced Recovery: Some users may feel that their body recovers faster after exercise or physical activity.
- Positive Mood: Some individuals may experience an improved sense of well-being and mood since MK-677 interacts with ghrelin receptors, which are primarily found in the brain and play a role in mood and pleasure.
Does MK-677 make you look younger?
MK-677 is not specifically designed to make you look younger, but some people may notice certain skin-related benefits when using it. MK-677 is a growth hormone secretagogue, which means it can increase the body’s production of growth hormones. Growth hormone is known to play a role in collagen production, which is essential for maintaining skin elasticity and firmness.
By boosting growth hormone levels, MK-677 may potentially improve the appearance of the skin, making it look healthier and more youthful. This can include reduced wrinkles and improved skin texture.
Does MK-677 mess with testosterone?
MK-677 does not directly affect testosterone levels. It is a growth hormone secretagogue, which means it promotes the production of growth hormones in the body. Growth hormone and testosterone are separate hormones with different functions.
What is a safe alternative to MK-677?
A safe alternative to MK-677 is to focus on natural methods to support overall health and fitness goals. Some alternatives include:
- Balanced Diet: Eating a nutritious diet that includes a variety of whole foods, lean proteins, healthy fats, and plenty of fruits and vegetables can support your body’s natural functions.
- Regular Exercise: Engaging in regular physical activity, such as cardiovascular exercises, strength training, or other forms of exercise, can help improve overall health and fitness.
- Proper Sleep: Getting enough quality sleep is essential for overall well-being, including muscle recovery and hormonal balance.
- Stress Management: Reducing chronic stress through relaxation techniques, meditation, or hobbies can positively impact health.
- Consult with Healthcare Provider: If you have specific health goals or concerns, talking to a healthcare provider can provide personalized guidance and advice on safe and effective approaches.
Does MK-677 increase bone size?
Yes, MK-677 may potentially increase bone size indirectly. MK-677 is a growth hormone secretagogue, which means it promotes the production of growth hormones in the body. Growth hormone plays a crucial role in the development and maintenance of bones and tissues.
By increasing growth hormone levels, MK-677 may support bone health and increase bone mineral density, which can lead to a potential increase in bone size and strength over time. However, the effects can vary among individuals, and MK-677 is not specifically intended for bone size enhancement.It is important to note that while some studies suggest potential benefits of MK-677 for immune function, more research is needed to understand its effects fully. Additionally, it is important to consult with a healthcare professional before taking any supplement or medication for immune system support.
Does MK-677 raise blood sugar?
Yes, MK-677 may raise blood sugar levels. MK-677 is a growth hormone secretagogue, which means it can increase the production of growth hormones in the body. One of the potential side effects of increased growth hormone levels is the elevation of blood sugar or glucose.
Is MK-677 anti-aging?
MK-677 is often considered to have potential anti-aging benefits. As a growth hormone secretagogue, it can increase the production of growth hormones in the body. Growth hormones are involved in various processes, including tissue repair, muscle growth, and metabolism. Some of these functions are associated with the aging process.
Does MK-677 affect cholesterol?
MK-677 may have some impact on cholesterol levels, but the effects can vary among individuals. MK-677 is a growth hormone secretagogue, which means it can increase the production of growth hormones in the body. Growth hormone is known to influence certain aspects of cholesterol metabolism.
In some cases, MK-677 has been reported to increase high-density lipoprotein cholesterol (HDL-C), which is often referred to as “good cholesterol” because it helps remove cholesterol from the blood vessels. However, it may not significantly affect total cholesterol and low-density lipoprotein cholesterol (LDL-C), often referred to as “bad cholesterol.”
Can a doctor prescribe MK-677?
Yes, a doctor can prescribe MK-677, but it’s essential to understand that MK-677 is not a typical medication or drug approved for most medical conditions. MK-677 is classified as a growth hormone secretagogue, which means it can increase the production of growth hormones in the body.
Does MK-677 lower insulin?
MK-677 may have the potential to influence insulin levels, but the effects can vary among individuals. MK-677 is a growth hormone secretagogue, which means it can increase the production of growth hormones in the body. Growth hormones can interact with insulin and affect how the body uses glucose (sugar).
In some cases, MK-677 has been reported to reduce insulin sensitivity, which means the body may require more insulin to regulate blood sugar levels. This can lead to higher insulin levels in the blood.
What happens if you take too much MK-677?
Taking too much MK-677 can lead to potential side effects and health risks. Since MK-677 is a growth hormone secretagogue, excessive intake may cause unnaturally high levels of growth hormone in the body, which can have various adverse effects.
Some of the possible side effects of taking too much MK-677 may include lethargy, joint pain, numbness, swelling, anxiety, and changes in blood sugar levels. Additionally, elevated levels of growth hormone for prolonged periods may have long-term effects on the body, including potential impacts on bone health, cardiovascular health, and hormone regulation.
Is MK-677 safer than steroids?
MK-677 is generally considered to be safer than traditional anabolic steroids. While both MK-677 and steroids may have an impact on muscle growth, they work through different mechanisms in the body.
MK-677 is a growth hormone secretagogue, which means it stimulates the production of growth hormones in the body. Growth hormone is essential for various physiological processes, including muscle growth, metabolism, and tissue repair. MK-677 does not directly introduce synthetic hormones into the body, and it does not significantly interfere with the body’s natural hormonal balance.
On the other hand, anabolic steroids are synthetic variations of testosterone, and their use can lead to a range of potential side effects, including hormonal imbalances, liver damage, cardiovascular issues, mood swings, and fertility problems, among others. Misuse or abuse of steroids can significantly increase these risks.
Overall, MK-677 is considered to be safer than steroids. However, it is important to note that both substances can have side effects, and it is important to talk to your doctor before taking either one.
How much muscle will I gain on MK-677?
The amount of muscle gained on MK-677 varies from person to person and depends on factors like diet, exercise, and individual response to the compound.
How much MK-677 should I take a day?
The recommended dosage of MK-677 is typically around 10-25mg per day, but it’s essential to follow the specific instructions and guidelines provided by the manufacturer or a healthcare professional.
Does MK-677 make you lean?
MK-677 can potentially help with reducing body fat and increasing muscle mass, which may contribute to a leaner physique in some individuals. MK-677 increases daily nitrogen balance in muscles by enhancing the body’s ability to retain and utilize nitrogen. This leads to a positive nitrogen balance, where the amount of nitrogen taken in exceeds the amount excreted. This favorable nitrogen balance promotes muscle protein synthesis and growth, supporting the development of lean muscle mass over time.
What are the results of MK-677 within 2 months?
Within 2 months of using MK-677, some users may experience improved recovery and increased muscle fullness. However, individual responses may vary. It’s essential to consult a healthcare professional before trying this new diet and study drug.
How long should you stay on MK-677?
The duration of MK-677 use varies based on individual goals and responses. Some people may use it for several months in cycles with breaks in between, while others may follow different protocols.
Can you eat after taking MK-677?
Yes, you can eat after taking MK-677. It is generally taken orally, and there are no specific restrictions on food intake after consumption.
Should I take MK-677 on rest days?
Taking MK-677 on rest days is a personal preference. It can be taken daily for consistent effects, but the timing can be adjusted to suit individual schedules.
Can MK-677 increase height?
MK-677 has been associated with an increase in growth hormone levels, but its impact on height in adults is not well-established. It’s not recommended for height increase in adults as the growth plates have typically closed.
Does MK-677 raise blood sugar?
Yes, MK-677 may increase blood sugar levels in some individuals. Diabetic individuals should use caution and consult with a healthcare professional before using MK-677.
How effective is MK-677?
MK-677 can be effective in increasing growth hormone levels and may have benefits such as improved muscle mass and recovery. However, its effectiveness can vary based on individual response and lifestyle factors.
Does ibutamoren affect testosterone?
Ibutamoren (MK-677) does not significantly affect testosterone levels, but it may increase other growth factors and hormones like IGF-1.
Can you mix MK-677 with juice?
Yes, MK-677 can be mixed with juice or other beverages for consumption, but it’s essential to follow the recommended dosage and instructions for accurate dosing.
Does MK-677 increase energy?
Some individuals may experience increased energy levels as a result of improved recovery and potential effects on growth hormones, but responses may vary.
What is the best stack for MK-677?
The ideal stack for MK-677 depends on individual goals, but it is often combined with other SARMs or compounds to enhance specific benefits like muscle growth or fat loss. Consulting a healthcare professional is advised for personalized advice.
How to prevent insulin resistance with MK-677?
To prevent or minimize the risk of insulin resistance while using MK-677, maintaining a balanced diet, regular exercise, and monitoring blood sugar levels are essential.
What is the alternative to MK-677?
MK-677 is a specific compound, and alternatives may not have identical effects. Other SARMs or compounds with different mechanisms of action might be considered alternatives for specific goals.
Does MK-677 stop testosterone?
MK-677 does not typically suppress testosterone levels. However, it’s essential to use it responsibly and consult a healthcare professional if you have concerns.
Is MK-677 a hormone?
MK-677 is not a hormone itself; it is a growth hormone secretagogue, meaning it stimulates the secretion of growth hormones in the body.
Why does MK-677 make you hungry?
MK-677 can increase appetite as a side effect, which is attributed to its influence on certain hormones that regulate hunger and satiety.
Can I eat after taking MK-677?
Yes, you can eat after taking MK-677. It is generally taken orally, and there are no specific restrictions on food intake after consumption.
Do you lose gains after MK-677?
The gains achieved while using MK-677 may be maintained with proper diet and training even after stopping the use of the compound, though individual results may vary.
Does MK-677 make you bulk?
MK-677 can contribute to increased muscle mass, but its effects may vary based on individual response and overall training and diet plan.
Is MK-677 bulk or cut?
MK-677 can be used for both bulking and cutting phases, depending on individual goals and how it is combined with other compounds.
How long is the MK 677 cycle?
MK-677 cycles can vary in length, but they are typically several weeks long, often ranging from 8 to 12 weeks. Consulting with a healthcare professional is recommended for personalized cycle planning.
What are the benefits of MK 677?
The potential benefits of MK-677 include increased muscle mass, improved recovery, enhanced bone density, and potential fat loss. Individual results may vary.
How to take MK-677 safely?
To take MK-677 safely, follow the recommended dosage and cycle guidelines provided by the manufacturer or a healthcare professional. Regular health monitoring is also essential.
Does MK-677 increase cortisol?
There is some evidence that MK-677 can increase cortisol levels.
Should you take MK-677 on an empty stomach?
Taking MK-677 on an empty stomach may enhance its absorption and effectiveness, but it’s essential to follow the specific instructions provided with the product.
How do I know if MK-677 is working?
While individual responses may vary, signs that MK-677 is working may include improved recovery, better sleep, increased food intake, and potential changes in muscle fullness.
What happens when you take MK-677?
When you take MK-677, it stimulates the secretion of growth hormone and insulin-like growth factor 1 (IGF-1), which may contribute to various potential physical benefits like muscle growth and recovery.
How long does it take for MK-677 to start working?
The effects of MK-677 may become noticeable within a few weeks, but individual response times can vary.
Does MK-677 affect fertility?
The impact of MK-677 on fertility is not well-studied in humans. It’s best to consult with a healthcare professional if you have concerns.
Does MK-677 need PCT?
MK-677 typically does not require post-cycle therapy (PCT) as it does not significantly suppress testosterone production.
How much HGH does MK-677 produce?
MK-677 does not directly produce HGH (human growth hormone), but it stimulates the release of growth hormone, which, in turn, may lead to increased levels of HGH.
When was MK-677 discovered?
MK-677, also known as Ibutamoren, was first developed in the mid-1990s.
Does MK-677 grow bones?
MK-677 has been associated with improved bone density and may have a positive impact on bone health in some individuals.
Does MK-677 increase stamina?
Improved stamina is one of the potential benefits reported by some users of MK-677, but individual responses can vary.
How much strength do you gain on MK-677?
MK-677 can contribute to increased strength, but the extent of strength gains can vary based on individual factors, training, and diet.
Should MK-677 be taken on an empty stomach?
Taking MK-677 on an empty stomach may enhance its absorption and effectiveness, but it’s essential to follow the specific instructions provided with the product.
Can you bulk with MK-677?
Yes, MK-677 can be used for bulking phases to support muscle growth and recovery when combined with appropriate training and nutrition.
What is best to stack with MK-677?
When should I start cutting?
The timing for starting a cutting phase depends on individual goals, current body composition, and desired target weight or physique.
Can you cut fat in 2 weeks?
A significant decrease in fat in just 2 weeks may be challenging and may not be sustainable. A healthy and gradual approach to fat loss is generally recommended for long-term results.
Can you gain muscle while cutting?
Gaining muscle while cutting (body recomposition) is possible, especially for beginners or those with higher body fat levels. However, it becomes more challenging as one gets closer to their genetic potential.
How fast do you see results with MK-677?
Individual responses to MK-677 can vary, but some users may start noticing certain effects within a few weeks of use.
Does MK-677 work immediately?
MK-677 does not work immediately, and it may take some time for its effects to become noticeable.
Does MK-677 speed healing?
MK-677 may potentially aid in the recovery process due to its impact on growth hormone levels, but it should not be used as a replacement for proper medical care for injuries.
How long is the MK677 cycle?
MK-677 cycles are typically several weeks long, often ranging from 8 to 12 weeks. It’s important to follow the specific guidelines provided by the manufacturer or a healthcare professional.
Blog

MK-677 for Muscle Growth and Strength
MK-677, also known as Ibutamoren, is a supplement that has gained popularity for its potential to promote muscle growth and enhance strength. By stimulating the release of growth hormone (GH) and insulin-like growth factor 1 (IGF-1), MK-677 may support anabolic processes and muscle hypertrophy.

MK-677 for Improved Sleep
MK-677, also known as Ibutamoren, is a supplement that has shown potential benefits in promoting improved sleep. Adequate sleep is essential for overall health and well-being, and MK-677 may offer a solution for individuals experiencing sleep difficulties.

Maximize Muscle Growth with MK-677
When it comes to maximizing muscle growth, fitness enthusiasts are constantly on the lookout for innovative approaches. One compound that has gained significant attention in recent years is MK-677, a growth hormone secretagogue. In this blog, We delve into something into the potential benefits of MK-677 and explore how it can be utilized to optimize muscle growth.

MK-677: Boost Your Fat Burning
If you’re on a mission to shed excess body fat, you may have heard about MK-677. In this blog, we explore how MK-677 can enhance your fat-burning journey and help you achieve your weight loss goals.

Unveiling the Impact: Side Effects of MK-677
MK-677 is a compound that has gained popularity in the fitness and bodybuilding community due to its potential to promote muscle growth and enhance bone density. However, like any other medication or supplement, it’s important to be aware of potential side effects. In this article, we will explore the possible side effects of MK-677 and provide you with valuable information to make informed decisions about its usage.

Ibutamoren MK-677: A Comprehensive Guide to Its Potential Benefits
Ibutamoren MK-677, also referred to as Nutrobal, is a type of SARM that has gained popularity due to its various potential benefits. In this article, we will review its benefits in detail.

MK-677: Unveiling Benefits & Side Effects!
MK-677, also known as Ibutamoren, is a synthetic compound classified as a growth hormone secretagogue. It has garnered attention for its potential as a performance-enhancing drug, boasting remarkable benefits in muscle growth, fat loss, and anti-aging properties.
18. Reference Sources and Summaries
- Meyer RM, Burgos-Robles A, Liu E, Correia SS, Goosens KA. A ghrelin-growth hormone axis drives stress-induced vulnerability to enhanced fear. Molecular psychiatry. 2014;19(12):1284-1294. doi:10.1038/mp.2013.135.
- Sun Y, Wang P, Zheng H, Smith RG. Ghrelin stimulation of growth hormone release and appetite is mediated through the growth hormone secretagogue receptor. Proceedings of the National Academy of Sciences of the United States of America. 2004;101(13):4679-4684.
doi:10.1073/pnas.0305930101. - Svensson J, Lönn L, Jansson JO, et al. Two-month treatment of obese subjects with the oral growth hormone (GH) secretagogue MK-677 increases GH secretion, fat-free mass, and energy expenditure. J Clin Endocrinol Metab. 1998;83(2):362-9.
- Welle S, Thornton C, Statt M, Mchenry B. Growth hormone increases muscle mass and strength but does not rejuvenate myofibrillar protein synthesis in healthy subjects over 60 years old. J Clin Endocrinol Metab. 1996;81(9):3239-43.
- Kim KR, Nam SY, Song YD, Lim SK, Lee HC, Huh KB. Low-dose growth hormone treatment with diet restriction accelerates body fat loss, exerts anabolic effect and improves growth hormone secretory dysfunction in obese adults. Horm Res. 1999;51(2):78-84.
- Welle S, Thornton C, Statt M, Mchenry B. Growth hormone increases muscle mass and strength but does not rejuvenate myofibrillar protein synthesis in healthy subjects over 60 years old. J Clin Endocrinol Metab. 1996;81(9):3239-43.
- Tavares ABW, Micmacher E, Biesek S, et al. Effects of Growth Hormone Administration on Muscle Strength in Men over 50 Years Old. International Journal of Endocrinology. 2013;2013:942030. doi:10.1155/2013/942030.
- Velloso CP. Regulation of muscle mass by growth hormone and IGF-I. British Journal of Pharmacology. 2008;154(3):557-568. doi:10.1038/bjp.2008.153.
- Weber MM. Effects of growth hormone on skeletal muscle. Horm Res. 2002;58 Suppl 3:43-8.
- Rennie M. Claims for the anabolic effects of growth hormone: a case of the Emperor’s new clothes? British Journal of Sports Medicine. 2003;37(2):100-105. doi:10.1136/bjsm.37.2.100.
- Johannsson G, Grimby G, Sunnerhagen KS, Bengtsson BA. Two years of growth hormone (GH) treatment increase isometric and isokinetic muscle strength in GH-deficient adults. J Clin Endocrinol Metab. 1997;82(9):2877-84.
- Harman SM, Blackman MR. The effects of growth hormone and sex steroid on lean body mass, fat mass, muscle strength, cardiovascular endurance and adverse events in healthy elderly women and men. Horm Res. 2003;60(Suppl 1):121-4.
- Norrelund H, Nair KS, Jorgensen JO, Christiansen JS, Moller N. The protein-retaining effects of growth hormone during fasting involve inhibition of muscle-protein breakdown. Diabetes. 2001;50(1):96-104.
- Adams GR.Insulin-like growth factorin muscle growth and its potential abuse by athletes. Western Journal of Medicine. 2001;175(1):7-9.
- Velloso CP. Regulation of muscle mass by growth hormone and IGF-I. British Journal of Pharmacology. 2008;154(3):557-568. doi:10.1038/bjp.2008.153.
- Christoffolete MA, Silva WJ, Ramos GV, et al. Muscle IGF-1-Induced Skeletal Muscle Hypertrophy Evokes Higher Insulin Sensitivity and Carbohydrate Use as Preferential Energy Substrate. BioMed Research International. 2015;2015:282984. doi:10.1155/2015/282984.
- Hamarneh SR, Murphy CA, Shih CW, et al. Relationship Between Serum IGF-1 and Skeletal Muscle IGF-1 mRNA Expression to Phosphocreatine Recovery After Exercise in Obese Men With Reduced GH. The Journal of Clinical Endocrinology and Metabolism. 2015;100(2):617-625.
doi:10.1210/jc.2014-2711. doi:10.1210/jc.2014-2711. - Heszele MF, Price SR. Insulin-like growth factor I: the yin and yang of muscle atrophy. Endocrinology. 2004;145(11):4803-5.
- Shavlakadze T, Chai J, Maley K, et al. A growth stimulus is needed for IGF-1 to induce skeletal muscle hypertrophy in vivo. J Cell Sci. 2010;123(Pt 6):960-71.
- Zou Y, Dong Y, Meng Q, Zhao Y, Li N. Incorporation of a skeletal muscle-specific enhancer in the regulatory region of Igf1 upregulates IGF1 expression and induces skeletal muscle hypertrophy. Scientific Reports. 2018;8:2781. doi:10.1038/s41598-018-21122-5.
- Available athttps://eurapa.biomedcentral.com/articles/10.1007/s11556-007-0022-1#:~:text=IGF%2DI%20has%20been%20implicated%20in%20the%20loss%20of%20muscle,than%20noncarriers%20with%20strength%20training..
- Ye F, Mathur S, Liu M, et al. Overexpression of insulin-like growth factor-1 attenuates skeletal muscle damage and accelerates muscle regeneration and functional recovery after disuse. Exp Physiol. 2013;98(5):1038-52.
- Murphy MG, Plunkett LM, Gertz BJ, et al. MK-677, an orally active growth hormone secretagogue, reverses diet-induced catabolism. J Clin Endocrinol Metab. 1998;83(2):320-5.
- Adunsky A, Chandler J, Heyden N, et al. MK-0677 (ibutamoren mesylate) for the treatment of patients recovering from hip fracture: a multicenter, randomized, placebo-controlled phase IIb study. Arch Gerontol Geriatr. 2011;53(2):183-9.
- Nass R, Pezzoli SS, Oliveri MC, et al. Effects of an oral ghrelin mimetic on body composition and clinical outcomes in healthy older adults: a randomized trial. Ann Intern Med. 2008;149(9):601-11.
- Chapman IM, Pescovitz OH, Murphy G, et al. Oral administration of growth hormone (GH) releasing peptide-mimetic MK-677 stimulates the GH/insulin-like growth factor-I axis in selected GH-deficient adults. J Clin Endocrinol Metab. 1997;82(10):3455-63.
- Svensson J, Ohlsson C, Jansson JO, et al. Treatment with the oral growth hormone secretagogue MK-677 increases markers of bone formation and bone resorption in obese young males. J Bone Miner Res. 1998;13(7):1158-66.
- Murphy MG, Bach MA, Plotkin D, et al. Oral administration of the growth hormone secretagogue MK-677 increases markers of bone turnover in healthy and functionally impaired elderly adults. The MK-677 Study Group. J Bone Miner Res. 1999;14(7):1182-8.
- Murphy MG, Weiss S, Mcclung M, et al. Effect of alendronate and MK-677 (a growth hormone secretagogue), individually and in combination, on markers of bone turnover and bone mineral density in postmenopausal osteoporotic women. J Clin Endocrinol Metab.
2001;86(3):1116-25. - Bach, M. A., Rockwood, K., Zetterberg, C., Thamsborg, G., Hébert, R., Devogelaer, J. P., Christiansen, J. S., Rizzoli, R., Ochsner, J. L., Beisaw, N., Gluck, O., Yu, L., Schwab, T., Farrington, J., Taylor, A. M., Ng, J., Fuh, V., & MK 0677 Hip Fracture
Study Group (2004). The effects of MK-0677, an oral growth hormone secretagogue, in patients with hip fracture. Journal of the American Geriatrics Society, 52(4), 516–523.https://doi.org/10.1111/j.1532-5415.2004.52156.x.. - Devin, J. K., Vaughan, D. E., Blevins, L. S., Jr, Chen, Q., Covington, J., Verity, D. K., & Young, P. P. (2008). Low-dose growth hormone administration mobilizes endothelial progenitor cells in healthy adults. Growth hormone & IGF research : official
journal of the Growth Hormone Research Society and the International IGF Research Society, 18(3), 253–263.https://doi.org/10.1016/j.ghir.2007.11.001.. - Eriksen EF, Kassem M, Langdahl B. Growth hormone, insulin-like growth factors and bone remodelling. Eur J Clin Invest. 1996;26(7):525-34.
- Ohlsson C, Bengtsson BA, Isaksson OG, Andreassen TT, Slootweg MC. Growth hormone and bone. Endocr Rev. 1998;19(1):55-79.
- Olney RC. Regulation of bone mass by growth hormone. Med Pediatr Oncol. 2003;41(3):228-34.
- Bex M, Bouillon R. Growth hormone and bone health. Horm Res. 2003;60 Suppl 3:80-6.
- Tritos NA, Klibanski A. Effects of Growth Hormone on Bone. Prog Mol Biol Transl Sci. 2016;138:193-211.
- Kuzma M, Payer J. [Growth hormone deficiency, its influence on bone mineral density and risk of osteoporotic fractures]. Cas Lek Cesk. 2010;149(5):211-6.
- Lindsey RC, Mohan S. Skeletal Effects of Growth Hormone and Insulin-like Growth Factor-I Therapy. Molecular and cellular endocrinology. 2016;432:44-55. doi:10.1016/j.mce.2015.09.017.
- Bouillon R. Growth hormone and bone. Horm Res. 1991;36 Suppl 1:49-55.
- Capozzi A, Casa SD, Altieri B, Pontecorvi A. Low bone mineral density in a growth hormone deficient (GHD) adolescent. Clinical Cases in Mineral and Bone Metabolism. 2013;10(3):203-205.
- Gillberg P, Mallmin H, Petrén-mallmin M, Ljunghall S, Nilsson AG. Two years of treatment with recombinant human growth hormone increases bone mineral density in men with idiopathic osteoporosis. J Clin Endocrinol Metab. 2002;87(11):4900-6.
- Aloia JF, Zanzi I, Ellis K, et al. Effects of growth hormone in osteoporosis. J Clin Endocrinol Metab. 1976;43(5):992-9.
- Colao A, Di somma C, Pivonello R, et al. Bone loss is correlated to the severity of growth hormone deficiency in adult patients with hypopituitarism. J Clin Endocrinol Metab. 1999;84(6):1919-24.
- Krantz E, Trimpou P, Landin-wilhelmsen K. Effect of Growth Hormone Treatment on Fractures and Quality of Life in Postmenopausal Osteoporosis: A 10-Year Follow-Up Study. J Clin Endocrinol Metab. 2015;100(9):3251-9.
- Fall C, Hindmarsh P, Dennison E, Kellingray S, Barker D, Cooper C. Programming of growth hormone secretion and bone mineral density in elderly men: a hypothesis. J Clin Endocrinol Metab. 1998;83(1):135-9.
- Rosen CJ. IGF-I and osteoporosis. Clin Lab Med. 2000;20(3):591-602.
- Kawai M, Rosen CJ. The Insulin-Like Growth Factor System in Bone: Basic and Clinical Implications. Endocrinology and metabolism clinics of North America. 2012;41(2):323-vi. doi:10.1016/j.ecl.2012.04.013.
- Niu T, Rosen CJ. The insulin-like growth factor-I gene and osteoporosis: a critical appraisal. Gene. 2005;361:38-56.
- Chen Y-C, Zhang L, Li E-N, et al. Association of the insulin-like growth factor-1 single nucleotide polymorphisms rs35767, rs2288377, and rs5742612 with osteoporosis risk: A meta-analysis. Pany. S, ed. Medicine. 2017;96(51):e9231. doi:10.1097/MD.0000000000009231.
- Vittorio Locatelli and Vittorio E. Bianchi, “Effect of GH/IGF-1 on Bone Metabolism and Osteoporsosis,” International Journal of Endocrinology, vol. 2014, Article ID 235060, 25 pages, 2014.https://doi.org/10.1155/2014/235060
- Kurland ES, Rosen CJ, Cosman F, et al. Insulin-like growth factor-I in men with idiopathic osteoporosis. J Clin Endocrinol Metab. 1997;82(9):2799-805.
- Sroga GE, Wu PC, Vashishth D. Insulin-like growth factor 1, glycation and bone fragility: implications for fracture resistance of bone. PLoS ONE. 2015;10(1):e0117046.
- Vandenput L, Sjögren K, Svensson J, Ohlsson C. The Role of IGF-1 for Fracture Risk in Men. Frontiers in Endocrinology. 2012;3:51. doi:10.3389/fendo.2012.00051.
- Ertuğrul I, Karan MA, Karan A, et al. Relationship between insulin-like growth factor 1 and bone mineral density in men aged over 65 years. Med Princ Pract. 2003;12(4):231-6.
- Gao S, Lv Z, Zhou C, Mao C, Sheng W. Association between IGF-1 polymorphisms and risk of osteoporosis in Chinese population: a meta-analysis. BMC Musculoskeletal Disorders. 2018;19:141. doi:10.1186/s12891-018-2066-y.
- Liu JM, Zhao HY, Ning G, et al. IGF-1 as an early marker for low bone mass or osteoporosis in premenopausal and postmenopausal women. J Bone Miner Metab. 2008;26(2):159-64.
- Copinschi G, Leproult R, Van onderbergen A, et al. Prolonged oral treatment with MK-677, a novel growth hormone secretagogue, improves sleep quality in man. Neuroendocrinology. 1997;66(4):278-86.
- Nass R, Pezzoli SS, Oliveri MC, et al. Effects of an Oral Ghrelin Mimetic on Body Composition and Clinical Outcomes in Healthy Older Adults: A Randomized, Controlled Trial. Annals of internal medicine. 2008;149(9):601-611.
- Frieboes RM, Murck H, Maier P, Schier T, Holsboer F, Steiger A. Growth hormone-releasing peptide-6 stimulates sleep, growth hormone, ACTH and cortisol release in normal man. Neuroendocrinology. 1995;61(5):584-9.
- Moreno-Reyes R, Kerkhofs M, L’hermite-balériaux M, Thorner MO, Van Cauter E, Copinschi G. Evidence against a role for the growth hormone-releasing peptide axis in human slow-wave sleep regulation. Am J Physiol. 1998;274(5 Pt 1): E779-84.
- Frieboes RM, Murck H, Antonijevic IA, Steiger A. Effects of growth hormone-releasing peptide-6 on the nocturnal secretion of GH, ACTH and cortisol and on the sleep EEG in man: role of routes of administration. J Neuroendocrinol. 1999;11(6):473-8.
- Morselli LL, Nedeltcheva A, Leproult R, et al. Impact of growth hormone replacement therapy on sleep in adult patients with growth hormone deficiency of pituitary origin. European journal of endocrinology/European Federation of Endocrine Societies. 2013;168(5):10.1530/EJE-12-1037.
doi:10.1530/EJE-12-1037. - Haqq AM, Stadler DD, Jackson RH, Rosenfeld RG, Purnell JQ, Lafranchi SH. Effects of growth hormone on pulmonary function, sleep quality, behavior, cognition, growth velocity, body composition, and resting energy expenditure in Prader-Willi syndrome. J
Clin Endocrinol Metab. 2003;88(5):2206-12. - Van cauter E, Copinschi G. Interrelationships between growth hormone and sleep. Growth Horm IGF Res. 2000;10 Suppl B:S57-62.
- Copinschi G, Nedeltcheva A, Leproult R, et al. Sleep disturbances, daytime sleepiness, and quality of life in adults with growth hormone deficiency. J Clin Endocrinol Metab. 2010;95(5):2195-202.
- Davidson JR, Moldofsky H, Lue FA. Growth hormone and cortisol secretion in relation to sleep and wakefulness. Journal of Psychiatry and Neuroscience. 1991;16(2):96-102.
- Moreno-reyes R, Kerkhofs M, L’hermite-balériaux M, Thorner MO, Van cauter E, Copinschi G. Evidence against a role for the growth hormone-releasing peptide axis in human slow-wave sleep regulation. Am J Physiol. 1998;274(5 Pt 1):E779-84.
- Shah N, Rice T, Tracy D, et al. Sleep and Insulin-Like Growth Factors in the Cardiovascular Health Study. Journal of Clinical Sleep Medicine : JCSM : Official Publication of the American Academy of Sleep Medicine. 2013;9(12):1245-1251. doi:10.5664/jcsm.3260.
- Mysliwiec V, Gill J, Matsangas P, Baxter T, Barr T, Roth BJ. IGF-1: a potential biomarker for efficacy of sleep improvement with automatic airway pressure therapy for obstructive sleep apnea?. Sleep Breath. 2015;19(4):1221-8.
- Izumi S, Ribeiro-filho FF, Carneiro G, Togeiro SM, Tufik S, Zanella MT. IGF-1 Levels are Inversely Associated With Metabolic Syndrome in Obstructive Sleep Apnea. J Clin Sleep Med. 2016;12(4):487-93.
- Izumi S, Ribeiro-Filho FF, Carneiro G, Togeiro SM, Tufik S, Zanella MT. IGF-1 Levels are Inversely Associated With Metabolic Syndrome in Obstructive Sleep Apnea. Journal of Clinical Sleep Medicine : JCSM : Official Publication of the American Academy
of Sleep Medicine. 2016;12(4):487-493. doi:10.5664/jcsm.5672. - Rusch HL, Gill JM. Effect of Acute Sleep Disturbance and Recovery on Insulin-Like Growth Factor-1 (IGF-1): Possible Connections and Clinical Implications. Journal of Clinical Sleep Medicine : JCSM : Official Publication of the American Academy of Sleep
Medicine. 2015;11(10):1245-1246. doi:10.5664/jcsm.5108. - Prinz PN, Moe KE, Dulberg EM, et al. Higher plasma IGF-1 levels are associated with increased delta sleep in healthy older men. J Gerontol A Biol Sci Med Sci. 1995;50(4):M222-6.
- Damanti S, Bourron O, Doulazmi M, et al. Relationship between sleep parameters, insulin resistance and age-adjusted insulin like growth factor-1 score in non diabetic older patients. Blondeau B, ed. PLoS ONE. 2017;12(4):e0174876. doi:10.1371/journal.pone.0174876.
- Obál F, Kapás L, Gardi J, Taishi P, Bodosi B, Krueger JM. Insulin-like growth factor-1 (IGF-1)-induced inhibition of growth hormone secretion is associated with sleep suppression. Brain Res. 1999;818(2):267-74.
- Chennaoui M, Drogou C, Sauvet F, Gomez-merino D, Scofield DE, Nindl BC. Effect of acute sleep deprivation and recovery on Insulin-like Growth Factor-I responses and inflammatory gene expression in healthy men. Eur Cytokine Netw. 2014;25(3):52-7.
- Rasmussen MH, Wildschiødtz G, Juul A, Hilsted J. Polysomnographic sleep, growth hormone insulin-like growth factor-I axis, leptin, and weight loss. Obesity (Silver Spring). 2008;16(7):1516-21.
- Levada OA, Troyan AS. Insulin-like growth factor-1: a possible marker for emotional and cognitive disturbances, and treatment effectiveness in major depressive disorder. Annals of General Psychiatry. 2017;16:38. doi:10.1186/s12991-017-0161-3.
- Peterfi Z, McGinty D, Sarai E, Szymusiak R. Growth hormone-releasing hormone activates sleep regulatory neurons of the rat preoptic hypothalamus. American Journal of Physiology – Regulatory, Integrative and Comparative Physiology. 2010;298(1):R147-R156.
doi:10.1152/ajpregu.00494.2009. - Cordido F, Peñalva A, Dieguez C, Casanueva FF. Massive growth hormone (GH) discharge in obese subjects after the combined administration of GH-releasing hormone and GHRP-6: evidence for a marked somatotroph secretory capability in obesity. J Clin Endocrinol
Metab. 1993;76(4):819-23. - Cordido F, Peñalva A, Peino R, Casanueva FF, Dieguez C. Effect of combined administration of growth hormone (GH)-releasing hormone, GH-releasing peptide-6, and pyridostigmine in normal and obese subjects. Metab Clin Exp. 1995;44(6):745-8.
- Copinschi G, Leproult R, Van onderbergen A, et al. Prolonged oral treatment with MK-677, a novel growth hormone secretagogue, improves sleep quality in man. Neuroendocrinology. 1997;66(4):278-86.
- Diekelmann S. Sleep for cognitive enhancement. Frontiers in Systems Neuroscience. 2014;8:46. doi:10.3389/fnsys.2014.00046.
- Aleman A, Verhaar HJ, De haan EH, et al. Insulin-like growth factor-I and cognitive function in healthy older men. J Clin Endocrinol Metab. 1999;84(2):471-5.
- Baker LD, Barsness SM, Borson S, et al. Effects of Growth Hormone–Releasing Hormone on Cognitive Function in Adults With Mild Cognitive Impairment and Healthy Older Adults: Results of a Controlled Trial. Archives of neurology. 2012;69(11):1420-1429. doi:10.1001/archneurol.2012.1970.
- Alvarez A, Cacabelos R, Sanpedro C, García-Fantini M, Aleixandre M. Serum TNF-alpha levels are increased and correlate negatively with free IGF-I in Alzheimer’s disease. Neurobiol Aging. 2007;28(4):533–536.
- Luppi C, Fioravanti M, Bertolini B, et al. Growth factors decrease in subjects with mild to moderate Alzheimer’s disease (AD): potential correction with dehydroepiandrosterone-sulfate (DHEAS) Arch Gerontol Geriatr. 2009;49(suppl 1):173–184.
- Aleman A, Torres-Alemán I. Circulating insulin-like growth factor I and cognitive function: neuromodulation throughout the lifespan. Prog Neurobiol. 2009;89(3):256–265.
- van Dam PS, Aleman A. Insulin-like growth factor-I, cognition and brain aging. Eur J Pharmacol. 2004;490(1–3):87–95.
- Rollero A, Murialdo G, Fonzi S, et al. Relationship between cognitive function, growth hormone and insulin-like growth factor I plasma levels in aged subjects. Neuropsychobiology. 1998;38(2):73–79.
- Frago LM, Pañeda C, Dickson SL, Hewson AK, Argente J, Chowen JA. Growth hormone (GH) and GH-releasing peptide-6 increase brain insulin-like growth factor-I expression and activate intracellular signalling pathways involved in neuroprotection. Endocrinology.
2002;143(10):4113-22. - Baserga R, Hongo A, Rubini M, Prisco M, Valentini SB 1997 The IGF-I receptor in cell growth, transformation and apoptosis. Biochim Biophys Acta 1332:F105–F126.
- Kulik G, Klippel A, Weber MJ 1997 Antiapoptotic signaling by the insulin-like growth factor I receptor, phosphatidylinositol 3-kinase and Akt. Mol Cell Biol 17:1595–1606.
- Chrysis D, Calikoglu AS, Ye P, D’Ercole AJ 2001 Insulin-like growth factor-I overexpression attenuates cerebellar apoptosis by altering the expression of Bcl family proteins in a developmentally specific manner. J Neurosci 21:1481–1489.
- Alessi DR, Andjelkovic M, Caudwell B, Cron P, Morrice N, Cohen P, Hemmings BA 1996 Mechanism of activation of protein kinase B by insulin and IGF-1. EMBO J 15:6541–6551.
- Dudek H, Datta SR, Franke TF, Birnbaum MJ, Yao R, Cooper GM, Segal RA, Kaplan DR, Greenberg ME 1997 Regulation of neural survival by the serine-threonine protein kinase Akt. Science 275:661–668.
- Mehrhof FB, Muller FU, Bergmann MW, Li P, Wang Y, Schmitz W, Dietz R, von Harsdorf R 2001 In cardiomyocyte hypoxia, insulin-like growth factor-I-induced antiapoptotic signaling requires phosphatidylinositol-3-OH-kinase-dependent and mitogen-activated
protein kinase-dependent activation of the transcription factor cAMP response element-binding protein. Circulation 104:2088–2094 - Gleichmann M, Weller M, Schuyltz JB 2000 Insulin-like growth factor-1-mediated protection from neuronal apoptosis is linked to phosphorylation of the pro-apoptotic protein BAD but not to inhibition of cytochrome c translocation in rat cerebellar neurons.
Neurosci Lett 282:69–72 - Peruzzi F, Prisco M, Dews M, Salomoni P, Grassilli E, Romano G, Calabretta B, Baserga R 1999 Multiple signaling pathways of the insulin-like growth factor 1 receptor in protection from apoptosis. Mol Cell Biol 19:7203–7215.
- Kulik G, Weber MJ 1998 Akt-dependent and -independent survival signaling pathways utilized by insulin-like growth factor I. Mol Cell Biol 18:6711–6718.
- Harada H, Andersen JS, Mann M, Terada N, Korsmeyer SJ 2001 p70S6 kinase signals cell survival as well as growth, inactivating the pro-apoptotic molecule BAD. Proc Natl Acad Sci USA 98:9666–9670.
- Desbois-Moutho C, Cadoret A, Blivet-Van Eggelpoel MJ, Bertrand F, Cherqui G, Perret C, Capeau J 2001 Insulin and IGF-1 stimulate the β-catenin pathway through two signalling cascades involving GSK-3β inhibition and Ras activation. Oncogene 20:252–259
- Park BC, Kido Y, Accili D 1999 Differential signaling of insulin and IGF-1 receptors to glycogen synthesis in murine hepatocytes. Biochemistry 38:7517–7523
- Cui H, Meng Y, Bulleit RF 1998 Inhibition of glycogen synthase kinase 3β activity regulates proliferation of cultured cerebellar granule cells. Brain Res Dev Brain Res 111:177–188.
- Tamatani M, Ogawa S, Nuñez G, Tokyama M 1998 Growth factors prevent changes in Bcl-2 and Bax expression and neuronal apoptosis induced by nitric oxide. Cell Death Differ 5:911–919
- Baker NlL, Carlo Russo V, Bernard O, D’Ercole AJ, Werther GA 1999 Interactions between bcl-2 and the IGF-I system control apoptosis in the developing mouse brain. Brain Res Dev Brain Res 118:109–118.
- Du K, Montminy M 1998 CREB is a regulatory target for the protein kinase Akt/PKB. J Biol Chem 273:32377.
- Pugazhenthi S, Nesterova A, Sable C, Heidenreich KA, Boxer LM, Heasly LE, Reusch JE 2000 Akt/protein kinase B upregulates Bcl-2 expression through cAMP-response element-binding protein. J Biol Chem 275:10761–10766.
- Kim SW, Her SJ, Park SJ, et al. Ghrelin stimulates proliferation and differentiation and inhibits apoptosis in osteoblastic MC3T3-E1 cells. Bone. 2005;37(3):359-69.
- Kim YS, Choi DH, Block ML, et al. A pivotal role of matrix metalloproteinase-3 activity in dopaminergic neuronal degeneration via microglial activation. FASEB J. 2007;21(1):179-87.
- Banks WA, Tschöp M, Robinson SM, Heiman ML. Extent and direction of ghrelin transport across the blood-brain barrier is determined by its unique primary structure. J Pharmacol Exp Ther. 2002;302(2):822-7.
- Chung H, Seo S, Moon M, Park S. Phosphatidylinositol-3-kinase/Akt/glycogen synthase kinase-3 beta and ERK1/2 pathways mediate protective effects of acylated and unacylated ghrelin against oxygen-glucose deprivation-induced apoptosis in primary rat cortical
neuronal cells. J Endocrinol. 2008;198(3):511-21. - García-cáceres C, Lechuga-sancho A, Argente J, Frago LM, Chowen JA. Death of hypothalamic astrocytes in poorly controlled diabetic rats is associated with nuclear translocation of apoptosis inducing factor. J Neuroendocrinol. 2008;20(12):1348-60
- Frago LM, Pañeda C, Dickson SL, Hewson AK, Argente J, Chowen JA. Growth hormone (GH) and GH-releasing peptide-6 increase brain insulin-like growth factor-I expression and activate intracellular signaling pathways involved in neuroprotection. Endocrinology.
2002;143(10):4113-22. - Nyberg F, Hallberg M. Growth hormone and cognitive function. Nat Rev Endocrinol. 2013;9(6):357-65.
- Baker LD, Barsness SM, Borson S, et al. Effects of Growth Hormone–Releasing Hormone on Cognitive Function in Adults With Mild Cognitive Impairment and Healthy Older Adults: Results of a Controlled Trial. Archives of neurology. 2012;69(11):1420-1429. doi:10.1001/archneurol.2012.1970.
- Maruff P, Falleti M. Cognitive function in growth hormone deficiency and growth hormone replacement. Horm Res. 2005;64 Suppl 3:100-8.
- Baker LD, Barsness SM, Borson S, et al. Effects of growth hormone–releasing hormone on cognitive function in adults with mild cognitive impairment and healthy older adults: results of a controlled trial. Arch Neurol. 2012;69(11):1420-9.
- Ong LK, Chow WZ, Tebay C, et al. Growth Hormone Improves Cognitive Function After Experimental Stroke. Stroke. 2018;49(5):1257-1266.
- Bove RM, White CC, Gerweck AV, et al. Effect of growth hormone on cognitive function in young women with abdominal obesity. Clinical endocrinology. 2016;84(4):635-637. doi:10.1111/cen.12996.
- Aleman A, Verhaar HJ, De haan EH, et al. Insulin-like growth factor-I and cognitive function in healthy older men. J Clin Endocrinol Metab. 1999;84(2):471-5.
- Sonntag WE, Deak F, Ashpole N, et al. Insulin-like growth factor-1 in CNS and cerebrovascular aging. Frontiers in Aging Neuroscience. 2013;5:27. doi:10.3389/fnagi.2013.00027.
- Nashiro K, Guevara-aguirre J, Braskie MN, et al. Brain Structure and Function Associated with Younger Adults in Growth Hormone Receptor-Deficient Humans. J Neurosci. 2017;37(7):1696-1707.
- Available at https://journals.lww.com/neurotodayonline/fulltext/2012/09200/Can_a_Growth_Hormone_Stimulating_Drug_Improve.6.aspx.
- Available at http://pediatrics.aappublications.org/content/142/4/e20173938.
- High WM, Briones-Galang M, Clark JA, et al. Effect of Growth Hormone Replacement Therapy on Cognition after Traumatic Brain Injury. Journal of Neurotrauma. 2010;27(9):1565-1575. doi:10.1089/neu.2009.1253.
- Grugni G, Sartorio A, Crinò A. Growth hormone therapy for Prader–willi syndrome: challenges and solutions. Therapeutics and Clinical Risk Management. 2016;12:873-881. doi:10.2147/TCRM.S70068.
- Xue Y, Gao Y, Wang S, Wang P. An examination of the effects of different doses of recombinant human growth hormone on children with growth hormone deficiency. Experimental and Therapeutic Medicine. 2016;11(5):1647-1652. doi:10.3892/etm.2016.3091.
- Lupien SB, Bluhm EJ, Ishii DN. Systemic insulin-like growth factor-I administration prevents cognitive impairment in diabetic rats, and brain IGF regulates learning/memory in normal adult rats. J Neurosci Res. 2003;74(4):512-23.
- Friedman SD, Baker LD, Borson S, et al. Growth hormone-releasing hormone effects on brain γ-aminobutyric acid levels in mild cognitive impairment and healthy aging. JAMA Neurol. 2013;70(7):883-90.
- Vitiello MV, Moe KE, Merriam GR, Mazzoni G, Buchner DH, Schwartz RS. Growth hormone releasing hormone improves the cognition of healthy older adults. Neurobiol Aging. 2006;27(2):318-23.
- Jeong YO, Shin SJ, Park JY, et al. MK-0677, a Ghrelin Agonist, Alleviates Amyloid Beta-Related Pathology in 5XFAD Mice, an Animal Model of Alzheimer’s Disease. Int J Mol Sci. 2018;19(6)
- Bajetto A, Barbero S, Bonavia R, et al. Stromal cell-derived factor-1α induces astrocyte proliferation through the activation of extracellular signal-regulated kinases 1/2 pathway. J Neurochem. 2001;77:1226–1236.
- Qui MS, Green SH. PC12 cell neuronal differentiation is associated with prolonged p21ras activity and consequent prolonged ERK activity. Neuron. 1992;9:705–717.
- Krapivinsky G, Krapivinsky L, Manasian Y, et al. The NMDA receptor is coupled to the ERK pathway by a direct interaction between NR2B and RasGRF1. Neuron. 2003;40:775–784.
- Alonso M, Viola H, Izquierdo I, Medina JH. Aversive experiences are associated with rapid and transient activation of ERKs in the rat hippocampus. Neurobiol Learn Mem. 2002;77:119–124.
- Raschke M, Kolbeck S, Bail H. Homologous growth hormone accelerates healing of segmental bone defects. Bone. 2001;4:368–373.
- Lal S, Wolf S, Herndon D. Growth hormone, burns and tissue healing. Growth Horm IGF Res. 2002;10:39–43.
- Ghofrani A, Holler D, Shulmann K. The influence of systemic growth hormone administration on the healing time of skin graft donor sites in a pig model. Plast Reconstr Surg. 1999;104:470–475.
- Mulligan K, Tai V, Schambelan M. Use of growth hormone and other anabolic agents in AIDS wasting. JPEN J Parenter Enteral Nutr. 1999;23:S202–S209.
- Pierre E, Perez-Polo J, Mitchell A. Insulin-like growth factor-1 liposomal gene transfer and systemic growth hormone stimulate wound healing. J Burn Care Rehabil. 1997;4:287–289.
- Biolo G, Fleming R, Wolfe R. Physiological hyperinsulinemia stimulates protein synthesis and enhances the transport of selected amino acids in human skeletal muscle. J Clin Invest. 1995;95:811–817.
- Zhang X, Chinkes D, Irtun O, Wolfe R. Anabolic insulin action on skin wound protein is augmented by exogenesis amino acids. Am J Physiol Endocrinol Metab. 2002;282:308–315.
- Coerper S, Wolf S, von Kiparski S, et al. Insulin-like growth factor accelerates gastric ulcer healing by stimulating cell proliferation and inhibiting gastric acid secretion. Scand J Gastroenterol. 2001;36:921–992.
- Lin E, Goncalves JA, Lowry SF. Efficacy of nutritional pharmacology in surgical patients. Curr Opin Clin Nutr Metab Care. 1998;1:41–50.
- Lieberman S, Bukar J, Chen S. Effects of recombinant human insulin-like growth in cachectic patients with the acquired immunodeficiency syndrome. J Clin Endocrinol Metab. 1994;78:404–410.
- Blumenfield I, Saiiyi S, Lanir Y. Enhancement of bone defect healing in old rats by TGF beta and IGF-1. Exp Gerontol. 2002;37:53–55.
- Hou YJ, Banerjee R, Thomas B, et al. SARM is required for neuronal injury and cytokine production in response to central nervous system viral infection. J Immunol. 2013;191(2):875-83.
- Johansson I, Destefanis S, Aberg ND, et al. Proliferative and protective effects of growth hormone secretagogues on adult rat hippocampal progenitor cells. Endocrinology. 2008;149(5):2191-9.
- Dioufa N, Schally AV, Chatzistamou I, et al. Acceleration of wound healing by growth hormone-releasing hormone and its agonists. Proc Natl Acad Sci USA. 2010;107(43):18611-5.
- Svensson J, Jansson JO, Ottosson M, et al. Treatment of obese subjects with the oral growth hormone secretagogue MK-677 affects serum concentrations of several lipoproteins, but not lipoprotein(a). J Clin Endocrinol Metab. 1999;84(6):2028-33.
- Baldanzi G, Filigheddu N, Cutrupi S, et al. Ghrelin and des-acyl ghrelin inhibit cell death in cardiomyocytes and endothelial cells through ERK1/2 and PI 3-kinase/AKT. The Journal of Cell Biology. 2002;159(6):1029-1037. doi:10.1083/jcb.200207165.
- ateishi K, et al. (2007) Human cardiac stem cells exhibit mesenchymal features and are maintained through Akt/GSK-3beta signaling. Biochem Biophys Res Commun 352(3):635–641.
- Choi SH, et al. (2013) Regulation of ROS-independent ERK signaling rescues replicative cellular senescence in ex vivo expanded human c-kit-positive cardiac progenitor cells. Int J Cardiol 169(1):73–82.
- Available at https://academic.oup.com/jcem/article/90/3/1864/2837042.
- Isgaard J. Cardiovascular disease and risk factors: the role of growth hormone. Horm Res. 2004;62 Suppl 4:31-8.
- Lombardi G, Colao A, Ferone D, et al. Effect of growth hormone on cardiac function. Horm Res. 1997;48 Suppl 4:38-42.
- Isgaard J, Arcopinto M, Karason K, Cittadini A. GH and the cardiovascular system: an update on a topic at heart. Endocrine. 2015;48(1):25-35. doi:10.1007/s12020-014-0327-6.
- Saccà L, Cittadini A, Fazio S. Growth hormone and the heart. Endocr Rev. 1994;15(5):555-73.
- Arcopinto M, Salzano A, Giallauria F, et al. Growth Hormone Deficiency Is Associated with Worse Cardiac Function, Physical Performance, and Outcome in Chronic Heart Failure: Insights from the T.O.S.CA. GHD Study. PLoS ONE. 2017;12(1):e0170058.
- De leonibus C, De marco S, Stevens A, Clayton P, Chiarelli F, Mohn A. Growth Hormone Deficiency in Prepubertal Children: Predictive Markers of Cardiovascular Disease. Horm Res Paediatr. 2016;85(6):363-71.
- Available at https://clinicaltrials.gov/ct2/show/NCT00397319.
- Liang S, Xue J, Li G. Effects of recombinant human growth hormone administration on cardiovascular risk factors in obese children with relative growth hormone deficiency. Lipids Health Dis. 2018;17(1):66.
- Available at https://link.springer.com/article/10.1007/s12020-016-1206-0.
- Ungvari Z, Csiszar A. The Emerging Role of IGF-1 Deficiency in Cardiovascular Aging: Recent Advances. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences. 2012;67A(6):599-610. doi:10.1093/gerona/gls072.
- Andreassen M, Raymond I, Kistorp C, Hildebrandt P, Faber J, Kristensen LØ. IGF1 as predictor of all cause mortality and cardiovascular disease in an elderly population. Eur J Endocrinol. 2009;160(1):25-31.
- Kaplan RC, Strickler HD, Rohan TE, Muzumdar R, Brown DL. Insulin-like growth factors and coronary heart disease. Cardiol Rev. 2005;13(1):35-9.
- Castellano G, Affuso F, Conza PD, Fazio S. The GH/IGF-1 Axis and Heart Failure. Current Cardiology Reviews. 2009;5(3):203-215. doi:10.2174/157340309788970306.
- Abdulle AM, Gillett MP, Abouchacra S, et al. Low IGF-1 levels are associated with cardiovascular risk factors in haemodialysis patients. Mol Cell Biochem. 2007;302(1-2):195-201.
- Córdova C, Boullosa DA, Custódio MR, et al. Atheroprotective Properties of Serum IGF-1 in the Carotid and Coronary Territories and Beneficial Role on the Physical Fitness of the Oldest Old. J Gerontol A Biol Sci Med Sci. 2016;71(10):1281-8.
- Wallander M, Norhammar A, Malmberg K, Ohrvik J, Rydén L, Brismar K. IGF binding protein 1 predicts cardiovascular morbidity and mortality in patients with acute myocardial infarction and type 2 diabetes. Diabetes Care. 2007;30(9):2343-8.
- Shah N, Rice T, Tracy D, et al. Sleep and Insulin-Like Growth Factors in the Cardiovascular Health Study. Journal of Clinical Sleep Medicine : JCSM : Official Publication of the American Academy of Sleep Medicine. 2013;9(12):1245-1251. doi:10.5664/jcsm.3260.
- González-guerra JL, Castilla-cortazar I, Aguirre GA, et al. Partial IGF-1 deficiency is sufficient to reduce heart contractibility, angiotensin II sensibility, and alter gene expression of structural and functional cardiac proteins. PLoS ONE. 2017;12(8):e0181760.
- Chigogora S, Zaninotto P, Kivimaki M, Steptoe A, Batty GD. Insulin-like growth factor 1 and risk of depression in older people: the English Longitudinal Study of Ageing. Transl Psychiatry. 2016;6(9):e898.
- Barton JS, Hindmarsh PC, Preece MA. Serum insulin-like growth factor 1 in congenital heart disease. Arch Dis Child. 1996;75(2):162-3.
- Giovannini S, Cesari M, Marzetti E, Leeuwenburgh C, Maggio M, Pahor M. EFFECTS OF ACE-INHIBITION ON IGF-1 AND IGFBP-3 CONCENTRATIONS IN OLDER ADULTS WITH HIGH CARDIOVASCULAR RISK PROFILE. The journal of nutrition, health & aging. 2010;14(6):457-460.
- Strazhesko ID, Tkacheva ON, Akasheva DU, et al. Growth Hormone, Insulin-Like Growth Factor-1, Insulin Resistance, and Leukocyte Telomere Length as Determinants of Arterial Aging in Subjects Free of Cardiovascular Diseases. Front Genet. 2017;8:198.
- Bergman D, Halje M, Nordin M, Engström W. Insulin-like growth factor 2 in development and disease: a mini-review. Gerontology. 2013;59(3):240-9.
- Touvron M, Escoubet B, Mericskay M, et al. Locally expressed IGF1 propeptide improves mouse heart function in induced dilated cardiomyopathy by blocking myocardial fibrosis and SRF-dependent CTGF induction. Dis Model Mech. 2012;5(4):481-91.
- Milman S, Atzmon G, Huffman DM, et al. Low insulin-like growth factor-1 level predicts survival in humans with exceptional longevity. Aging Cell. 2014;13(4):769-71.
- Zhang Z, et al. (2013) Rosuvastatin enhances the therapeutic efficacy of adipose-derived mesenchymal stem cells for myocardial infarction via PI3K/Akt and MEK/ERK pathways. Basic Res Cardiol 108(2):333.
- Sun X, Fang B, Zhao X, Zhang G, Ma H (2014) Preconditioning of mesenchymal stem cells by sevoflurane to improve their therapeutic potential. PLoS ONE 9(3):e90667.
- Gude N, et al. (2006) Akt promotes increased cardiomyocyte cycling and expansion of the cardiac progenitor cell population. Circ Res 99(4):381–388.
- Hahn JY, et al. (2008) Pre-treatment of mesenchymal stem cells with a combination of growth factors enhances gap junction formation, cytoprotective effect on cardiomyocytes, and therapeutic efficacy for myocardial infarction. J Am Coll Cardiol 51(9):933–943.
- Pasha Z, et al. (2008) Preconditioning enhances cell survival and differentiation of stem cells during transplantation in infarcted myocardium. Cardiovasc Res 77(1):134–142.
- Gude N, et al. (2006) Akt promotes increased cardiomyocyte cycling and expansion of the cardiac progenitor cell population. Circ Res 99(4):381–388.
- Kanashiro-Takeuchi RM, Schulman IH, Hare JM (2011) Pharmacologic and genetic strategies to enhance cell therapy for cardiac regeneration. J Mol Cell Cardiol 51(4):619–625.
- Fischer KM, et al. (2009) Enhancement of myocardial regeneration through genetic engineering of cardiac progenitor cells expressing Pim-1 kinase. Circulation 120(21):2077–2087.
- Kiaris H, Schally AV, Kalofoutis A (2005) Extrapituitary effects of the growth hormone-releasing hormone. Vitam Horm 70:1–24.
- Ciampani T, Fabbri A, Isidori A, Dufau ML (1992) Growth hormone-releasing hormone is produced by rat Leydig cell in culture and acts as a positive regulator of Leydig cell function. Endocrinology 131:2785–2792.
- Khorram O, Garthwaite M, Golos T (2001) The influence of aging and sex hormones on expression of growth hormone-releasing hormone in the human immune system. J Clin Endocrinol Metab 86:3157–3161.
- Florea V, Majid SS, Kanashiro-takeuchi RM, et al. Agonists of growth hormone-releasing hormone stimulate self-renewal of cardiac stem cells and promote their survival. Proc Natl Acad Sci USA. 2014;111(48):17260-5.
- Kanashiro-Takeuchi RM, et al. (2010) Cardioprotective effects of growth hormone-releasing hormone agonist after myocardial infarction. Proc Natl Acad Sci USA 107(6):2604–2609.
- Kanashiro-Takeuchi RM, et al. (2012) Activation of growth hormone releasing hormone (GHRH) receptor stimulates cardiac reverse remodeling after myocardial infarction (MI). Proc Natl Acad Sci USA 109(2):559–563.
- Cai R, et al. (2014) Synthesis of new potent agonistic analogs of growth hormone-releasing hormone (GHRH) and evaluation of their endocrine and cardiac activities. Peptides 52:104–112.
- Ma Y, Zhang L, Launikonis BS, Chen C. Growth hormone secretagogues preserve the electrophysiological properties of mouse cardiomyocytes isolated from in vitro ischemia/reperfusion heart. Endocrinology. 2012;153(11):5480-90.
- Frascarelli S, Ghelardoni S, Ronca-Testoni S, Zucchi R 2003 Effect of ghrelin and synthetic growth hormone secretagogues in normal and ischemic rat heart. Basic Res Cardiol 98:401–405.
- Chang L, Ren Y, Liu X, Li WG, Yang J, Geng B, Weintraub NL, Tang C 2004 Protective effects of ghrelin on ischemia/reperfusion injury in the isolated rat heart. J Cardiovasc Pharmacol 43:165–170.
- Zhang GG, Teng X, Liu Y, Cai Y, Zhou YB, Duan XH, Song JQ, Shi Y, Tang CS, Yin XH, Qi YF 2009 Inhibition of endoplasm reticulum stress by ghrelin protects against ischemia/reperfusion injury in rat heart. Peptides 30:1109–1116.
- Torsello A, Bresciani E, Rossoni G, Avallone R, Tulipano G, Cocchi D, Bulgarelli I, Deghenghi R, Berti F, Locatelli V 2003 Ghrelin plays a minor role in the physiological control of cardiac function in the rat. Endocrinology 144:1787–1792.
- Cittadini A, Grossman JD, Strömer H, Katz SE, Morgan JP, Douglas PS. Importance of an intact growth hormone/insulin-like growth factor 1 axis for normal post-infarction healing: studies in dwarf rats. Endocrinology. 2001;142(1):332-8.
- Waters MJ, Blackmore DG (2011) Growth hormone (GH), brain development and neural stem cells. Pediatr Endocrinol Rev 9(2):549–553.
- Khorram, M. Garthwaite, T. Golos. The influence of aging and sex hormones on expression of growth hormone-releasing hormone in the human immune system. J. Clin. Endocrinol. Metab., 86 (2001), pp. 3157-3161.
- Dialynas, H. Brown-Borg, A. Bartke. Immune function in transgenic mice overexpressing growth hormone (GH) releasing hormone, GH or GH antagonist. Proc. Soc. Exp. Biol. Med., 221 (1999), pp. 178-183.
- Dorshkind, N.D. Horseman. Anterior pituitary hormones, stress, and immune system homeostasis. Bioessays, 23 (2001), pp. 288-294.
- Burgess, et al. The immune–endocrine loop during aging: role of growth hormone and insulin-like growth factor-I. Neuroimmunomodulation, 6 (1999), pp. 56-68.
- C. Gelato. Aging and immune function: a possible role for growth hormone. Horm. Res., 45 (1996), pp. 46-49.
- L. Marshall, B. Perras, H.L. Fehm, J. Born. Changes in immune cell counts and interleukin (IL)-1beta production in humans after a somnogenically active growth hormone-releasing hormone (GHRH) administration. Brain Behav. Immun., 15 (2001), pp. 227-234.
- Hattori N. Expression, regulation and biological actions of growth hormone (GH) and ghrelin in the immune system. Growth Horm IGF Res. 2009;19(3):187-97.
- Masternak MM, Bartke A. Growth hormone, inflammation and aging. Pathobiology of Aging & Age Related Diseases. 2012;2:10.3402/pba.v2i0.17293. doi:10.3402/pba.v2i0.17293.
- Meazza C, Pagani S, Travaglino P, Bozzola M. Effect of growth hormone (GH) on the immune system. Pediatr Endocrinol Rev. 2004;1 Suppl 3:490-5.
- Rapaport R, Oleske J, Ahdieh H, Solomon S, Delfaus C, Denny T. Suppression of immune function in growth hormone-deficient children during treatment with human growth hormone. J Pediatr. 1986;109(3):434-9.
- Koo GC, Huang C, Camacho R, et al. Immune enhancing effect of a growth hormone secretagogue. J Immunol. 2001;166(6):4195-201.
- Morrhaye G, Kermani H, Legros J-J, et al. Impact of Growth Hormone (GH) Deficiency and GH Replacement upon Thymus Function in Adult Patients. Unutmaz D, ed. PLoS ONE. 2009;4(5):e5668. doi:10.1371/journal.pone.0005668.
- Gelato MC. Aging and immune function: a possible role for growth hormone. Horm Res. 1996;45(1-2):46-9.
- Available at https://www.nature.com/articles/pr1984567.
- Available at https://clinicaltrials.gov/ct2/show/NCT00071240.
- Alzaid A, Kim JH, Devlin RH, Martin SAM, Macqueen DJ. Growth hormone transgenesis in coho salmon disrupts muscle immune function impacting cross-talk with growth systems. J Exp Biol. 2018;221(Pt 13).
- Carroll PV, Christ ER, Bengtsson BA, et al. Growth hormone deficiency in adulthood and the effects of growth hormone replacement: a review. Growth Hormone Research Society Scientific Committee. J Clin Endocrinol Metab. 1998;83(2):382-95.
- Available at http://www.asja.eg.net/article.asp?issn=1687-7934;year=2016;volume=9;issue=2;spage=194;epage=200;aulast=Salem.
- Villares R, Kakabadse D, Juarranz Y, Gomariz RP, Martínez-a C, Mellado M. Growth hormone prevents the development of autoimmune diabetes. Proc Natl Acad Sci USA. 2013;110(48):E4619-27.
- Mazzoccoli G, Vendemiale G, De Cata A, Carughi S, Tarquini R. Altered time structure of neuro-endocrine-immune system function in lung cancer patients. BMC Cancer. 2010;10:314. doi:10.1186/1471-2407-10-314.
- Smith TJ. Insulin-Like Growth Factor-I Regulation of Immune Function: A Potential Therapeutic Target in Autoimmune Diseases? Pharmacological Reviews. 2010;62(2):199-236. doi:10.1124/pr.109.002469.
- Ge R-T, Mo L-H, Wu R, et al. Insulin-like growth factor-1 endues monocytes with immune suppressive ability to inhibit inflammation in the intestine. Scientific Reports. 2015;5:7735. doi:10.1038/srep07735.
- Bilbao D, Luciani L, Johannesson B, Piszczek A, Rosenthal N. Insulin-like growth factor-1 stimulates regulatory T cells and suppresses autoimmune disease. EMBO Molecular Medicine. 2014;6(11):1423-1435. doi:10.15252/emmm.201303376.
- Franz A-C, Faass O, Köllner B, et al. Endocrine and Local IGF-I in the Bony Fish Immune System. Dixon B, ed. Biology. 2016;5(1):9. doi:10.3390/biology5010009.
- Spadaro O, Camell C, Bosurgi L, et al. IGF1 shapes the macrophage activation in response to immunometabolic challenge. Cell reports. 2017;19(2):225-234. doi:10.1016/j.celrep.2017.03.046.
- Alzaid A, Castro R, Wang T, et al. Cross Talk Between Growth and Immunity: Coupling of the IGF Axis to Conserved Cytokine Pathways in Rainbow Trout. Endocrinology. 2016;157(5):1942-55.
- Rodrigues LS, Hacker MA, Illarramendi X, et al. Circulating levels of insulin-like growth factor-I (IGF-I) correlate with disease status in leprosy. BMC Infect Dis. 2011;11:339.
- Gelato MC. Aging and immune function: a possible role for growth hormone. Horm Res. 1996;45(1-2):46-9.
- Van bilsen K, Driessen GJ, De paus RA, et al. Low level IGF-1 and common variable immune deficiency: an unusual combination. Neth J Med. 2008;66(9):368-72.
- Rodrigues LS, Hacker MA, Illarramendi X, et al. Circulating levels of insulin-like growth factor-I (IGF-I) correlate with disease status in leprosy. BMC Infectious Diseases. 2011;11:339. doi:10.1186/1471-2334-11-339.
- Ge RT, Mo LH, Wu R, et al. Insulin-like growth factor-1 endues monocytes with immune suppressive ability to inhibit inflammation in the intestine. Sci Rep. 2015;5:7735.
- Puche JE, Castilla-Cortázar I. Human conditions of insulin-like growth factor-I (IGF-I) deficiency. Journal of Translational Medicine. 2012;10:224. doi:10.1186/1479-5876-10-224.
- Quentien MH, Delemer B, Papadimitriou DT, et al. Deficit in anterior pituitary function and variable immune deficiency (DAVID) in children presenting with adrenocorticotropin deficiency and severe infections. J Clin Endocrinol Metab. 2012;97(1):E121-8.
- Available at https://www.tandfonline.com/doi/abs/10.1586/eem.10.73.
- Tu W, Cheung PT, Lau YL. Insulin-like growth factor 1 promotes cord blood T cell maturation and inhibits its spontaneous and phytohemagglutinin-induced apoptosis through different mechanisms. J Immunol. 2000;165(3):1331-6
- Baatar D, Patel K, Taub DD. The effects of ghrelin on inflammation and the immune system. Mol Cell Endocrinol. 2011;340(1):44-58.
- Brown PA, Davis WC, Draghia-akli R. Immune-enhancing effects of growth hormone-releasing hormone delivered by plasmid injection and electroporation. Mol Ther. 2004;10(4):644-51.
- Available at https://www.researchgate.net/publication/326998293_Biological_activity_of_a_new_Growth_hormone_secretagogue_study_in_fish_and_murine_cell_line.
- Rubinek T, Rubinfeld H, Hadani M, Barkai G, Shimon I. Nitric oxide stimulates growth hormone secretion from human fetal pituitaries and cultured pituitary adenomas. Endocrine. 2005;28(2):209-16.
- Valverde I, Peñalva A, Ghigo E, Casanueva FF, Dieguez C. Involvement of nitric oxide in the regulation of growth hormone secretion in dogs. Neuroendocrinology. 2001;74(4):213-9.
- Rigamonti AE, Cella SG, Marazzi N, Müller EE. Nitric oxide modulation of the growth hormone-releasing activity of Hexarelin in young and old dogs. Metab Clin Exp. 1999;48(2):176-82.
- Doi SQ, Jacot TA, Sellitti DF, et al. Growth hormone increases inducible nitric oxide synthase expression in mesangial cells. J Am Soc Nephrol. 2000;11(8):1419-25.
- Available at http://erj.ersjournals.com/content/31/4/815.
- Deniz Tuncel, Fatma Inanc Tolun, and Ismail Toru, “Serum Insulin-Like Growth Factor-1 and Nitric Oxide Levels in Parkinson’s Disease,” Mediators of Inflammation, vol. 2009, Article ID 132464, 4 pages, 2009.
- Available at https://clinicaltrials.gov/ct2/show/NCT00470002.
- Böger RH , Skamira C , Bode-Böger SM , Brabant G , von zur Muhlen A , Frolich JC. 1996. Nitric oxide may mediate the hemodynamic effects of recombinant growth hormone in patients with acquired growth hormone deficiency. A double-blind, placebo-controlled
study. J Clin Invest 98:2706–2713. - Thum T , Fleissner F , Klink I , Tsikas D , Jakob M , Bauersachs J , Stichtenoth DO. 2007. Growth hormone treatment improves markers of systemic nitric oxide bioavailability via insulin-like growth factor-I. J Clin Endocrinol Metab 92:4172–4179.
- Mani maran RR, Sivakumar R, Ravisankar B, et al. Growth hormone directly stimulates testosterone and oestradiol secretion by rat Leydig cells in vitro and modulates the effects of LH and T3. Endocr J. 2000;47(2):111-8.
- Ho KY, Evans WS, Blizzard RM, et al. Effects of sex and age on the 24-hour profile of growth hormone secretion in man: importance of endogenous estradiol concentrations. J Clin Endocrinol Metab. 1987;64(1):51-8.
- Amitani M, Amitani H, Cheng K-C, et al. The Role of Ghrelin and Ghrelin Signaling in Aging. International Journal of Molecular Sciences. 2017;18(7):1511. doi:10.3390/ijms18071511.
- Minor RK, Chang JW, de Cabo R. Hungry for Life: How the arcuate nucleus and neuropeptide Y may play a critical role in mediating the benefits of calorie restriction. Molecular and cellular endocrinology. 2009;299(1):79-88. doi:10.1016/j.mce.2008.10.044.
- Babaei-Balderlou F, Khazali H. Effects of Ghrelin on Sexual Behavior and Luteinizing Hormone Beta-subunit Gene Expression in Male Rats . Journal of Reproduction & Infertility. 2016;17(2):88-96.
- https://www.sciencedaily.com/releases/2015/01/150127110955.htm.
- Brod M, Pohlman B, Højbjerre L, Adalsteinsson JE, Rasmussen MH. Impact of adult growth hormone deficiency on daily functioning and well-being. BMC Research Notes. 2014;7:813. doi:10.1186/1756-0500-7-813.
- Maggi M, Buvat J, Corona G, Guay A, Torres LO. Hormonal causes of male sexual dysfunctions and their management (hyperprolactinemia,thyroid disorders, GH disorders, and DHEA). J Sex Med. 2013;10(3):661-77.
- Ginzburg E, Lin A, Sigler M, Olsen D, Klimas N, Mintz A. Testosterone and growth hormone normalization: a retrospective study of health outcomes. Journal of multidisciplinary healthcare. 2008;1:79-86.
- Brod M, Højbjerre L, Adalsteinsson JE, Rasmussen MH. Assessing the impact of growth hormone deficiency and treatment in adults: development of a new disease-specific measure. J Clin Endocrinol Metab. 2014;99(4):1204-12.
- Available at https://www.researchgate.net/publication/12600670_Effects_of_growth_hormone_on_male_reproductive_functions.
- Galdiero M, Pivonello R, Grasso LF, Cozzolino A, Colao A. Growth hormone, prolactin, and sexuality. J Endocrinol Invest. 2012;35(8):782-94.
- Becker AJ, Uckert S, Stief CG, et al. Possible role of human growth hormone in penile erection. J Urol. 2000;164(6):2138-42.
- Becker AJ, Uckert S, Stief CG, et al. Serum levels of human growth hormone during different penile conditions in the cavernous and systemic blood of healthy men and patients with erectile dysfunction. Urology. 2002;59(4):609-14.
- Khorram O, Laughlin GA, Yen SS. Endocrine and metabolic effects of long-term administration of [Nle27]growth hormone-releasing hormone-(1-29)-NH2 in age-advanced men and women. J Clin Endocrinol Metab. 1997;82(5):1472-9.Gades NM, Jacobson DJ, McGree ME, et al. The associations between serum sex hormones, erectile function, and sex drive: the Olmsted County study of urinary symptoms and health status among men. The journal of sexual medicine. 2008;5(9):2209-2220. doi:10.1111/j.1743-6109.2008.00924.x.
- Otunctemur A, Ozbek E, Sahin S, et al. Low serum insulin-like growth factor-1 in patients with erectile dysfunction. Basic and Clinical Andrology. 2016;26:1. doi:10.1186/s12610-015-0028-x.
- Rajfer J. Growth Factors and Gene Therapy for Erectile Dysfunction. Reviews in Urology. 2000;2(1):34.
- Pastuszak AW, Liu JS, Vij A. IGF-1 levels are significantly correlated with patient-reported measures of sexual function. International journal of impotence research. 2011; 23(5):220-6.
- Pastuszak AW, Liu JS, Vij A, et al. IGF-1 levels are significantly correlated with patient-reported measures of sexual function. Int J Impot Res. 2011;23(5):220-6.
- El-Sakka AI, Lin CS, Chui RM, Dahiya R, Lue TF. Effects of diabetes on nitric oxide synthase and growth factor genes and protein expression in an animal model. Int J Impot Res. 1999;11:123–32. doi: 10.1038/sj.ijir.3900392.
- Soh J, Katsuyama M, Ushijima S, Mizutani Y, Kawauchi A, Yabe-Nishimura C, et al. Localization of increased insulin-like growth factor binding protein-3 in diabetic rat penis: Implications for erectile dysfunction. Urology. 2007;70:1019–23. doi: 10.1016/j.urology.2007.07.057.
- Pu XY, Zheng XG, Zhang Y, Xiao HJ, Xu ZP, Liu JM, et al. Higher expression of mRNA and protein of insulin-like growth factor binding protein-3 in old rat penile tissues: implications for erectile dysfunction. J Sex Med. 2011;8:2181–90. doi: 10.1111/j.1743-6109.2011.02318.x.
- Veldhuis JD, Erickson D, Wigham J, Weist S, Miles JM, Bowers CY. Gender, Sex-Steroid, and Secretagogue-Selective Recovery from Growth Hormone-Induced Feedback in Older Women and Men. The Journal of Clinical Endocrinology and Metabolism. 2011;96(8):2540-2547.
doi:10.1210/jc.2011-0298.You can read the full article at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3146792/
- Khorram O, Laughlin GA, Yen SS. Endocrine and metabolic effects of long-term administration of [Nle27]growth hormone-releasing hormone-(1-29)-NH2 in age-advanced men and women. J Clin Endocrinol Metab. 1997;82(5):1472-9.
- Nass R, Pezzoli SS, Oliveri MC, et al. Effects of an oral ghrelin mimetic on body composition and clinical outcomes in healthy older adults: a randomized trial. Ann Intern Med. 2008;149(9):601-11.
- Catalina PF, Mallo F, Andrade MA, García-mayor RV, Diéguez C. Growth hormone (GH) response to GH-releasing peptide-6 in type 1 diabetic patients with exaggerated GH-releasing hormone-stimulated GH secretion. J Clin Endocrinol Metab. 1998;83(10):3663-7.
- Jacks T, Smith R, Judith F, et al. MK-0677, a potent, novel, orally active growth hormone (GH) secretagogue: GH, insulin-like growth factor I, and other hormonal responses in beagles. Endocrinology. 1996;137(12):5284-9.
- Hickey GJ, Jacks TM, Schleim KD, et al. Repeat administration of the GH secretagogue MK-0677 increases and maintains elevated IGF-I levels in beagles. J Endocrinol. 1997;152(2):183-92.
- Schleim KD, Jacks T, Cunningham P, et al. Increases in circulating insulin-like growth factor I levels by the oral growth hormone secretagogue MK-0677 in the beagle are dependent upon pituitary mediation. Endocrinology. 1999;140(4):1552-8.
- Teppala S, Shankar A. Association Between Serum IGF-1 and Diabetes Among U.S. Adults. Diabetes Care. 2010;33(10):2257-2259. doi:10.2337/dc10-0770.
- Simpson HL, Umpleby AM, Russell-jones DL. Insulin-like growth factor-I and diabetes. A review. Growth Horm IGF Res. 1998;8(2):83-95.
- Friedrich N, Thuesen B, Jørgensen T, et al. The association between IGF-I and insulin resistance: a general population study in Danish adults. Diabetes Care. 2012;35(4):768-73.
- Palta M, LeCaire T, Sadek-Badawi M, Herrera V, Danielson KK. The trajectory of IGF-1 across age and duration of type 1 diabetes. Diabetes/metabolism research and reviews. 2014;30(8):777-783. doi:10.1002/dmrr.2554.
You can read the full article at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4236234/
- Aguirre GA, De Ita JR, de la Garza RG, Castilla-Cortazar I. Insulin-like growth factor-1 deficiency and metabolic syndrome. Journal of Translational Medicine. 2016;14:3. doi:10.1186/s12967-015-0762-z.
- Drogan D, Schulze MB, Boeing H, Pischon T. Insulin-Like Growth Factor 1 and Insulin-Like Growth Factor-Binding Protein 3 in Relation to the Risk of Type 2 Diabetes Mellitus: Results From the EPIC-Potsdam Study. Am J Epidemiol. 2016;183(6):553-60.
- Suda K, Matsumoto R, Fukuoka H, et al. The influence of type 2 diabetes on serum GH and IGF-I levels in hospitalized Japanese patients. Growth Horm IGF Res. 2016;29:4-10.
- Færch L, Juul A, Pedersen-Bjergaard U, Thorsteinsson B. Association of IGF1 with glycemic control and occurrence of severe hypoglycemia in patients with type 1 diabetes mellitus. Endocrine Connections. 2012;1(1):31-36. doi:10.1530/EC-12-0012.
- Chantelau E. Evidence that upregulation of serum IGF-1 concentration can trigger acceleration of diabetic retinopathy. Br J Ophthalmol. 1998;82(7):725-30.
- Fridlyand LE, Tamarina NA, Schally AV, Philipson LH. Growth Hormone-Releasing Hormone in Diabetes. Frontiers in Endocrinology. 2016;7:129. doi:10.3389/fendo.2016.00129.
- Johansen PB, Segev Y, Landau D, Phillip M, Flyvbjerg A. Growth hormone (GH) hypersecretion and GH receptor resistance in streptozotocin diabetic mice in response to a GH secretagogue. Exp Diabesity Res. 2003;4(2):73-81.
- Clark RG, Thomas GB, Mortensen DL, et al. Growth hormone secretagogues stimulate the hypothalamic-pituitary-adrenal axis and are diabetogenic in the Zucker diabetic fatty rat. Endocrinology. 1997;138(10):4316-23.
- Holly JM, Amiel SA, Sandhu RR, Rees LH, Wass JA. The role of growth hormone in diabetes mellitus. J Endocrinol. 1988;118(3):353-64.
- Nazaimoon WM, Ng ML, Khalid BA. Fasting growth hormone levels in diabetes mellitus. Ann Acad Med Singap. 1993;22(6):861-3.
- Wurzburger MI, Prelevic GM, Sonksen PH, Balint-peric L. Growth hormone levels in patients with type 1 diabetes are age related. Diabet Med. 1993;10(2):159-61.
- Kim S-H, Park M-J. Effects of growth hormone on glucose metabolism and insulin resistance in human. Annals of Pediatric Endocrinology & Metabolism. 2017;22(3):145-152. doi:10.6065/apem.2017.22.3.145.
- Luger A, Mattsson AF, Koltowska-häggström M, et al. Incidence of diabetes mellitus and evolution of glucose parameters in growth hormone-deficient subjects during growth hormone replacement therapy: a long-term observational study. Diabetes Care.
2012;35(1):57-62. - Del guercio MJ, Di natale B, Gargantini L, Garlaschi C, Chiumello G. Effect of somatostatin on blood sugar, plasma growth hormone, and glucagon levels in diabetic children. Diabetes. 1976;25(7):550-3.
- Bonfig W, Molz K, Woelfle J, et al. Metabolic safety of growth hormone in type 1 diabetes and idiopathic growth hormone deficiency. J Pediatr. 2013;163(4):1095-8.e4.
- Jeffcoate W. Growth hormone therapy and its relationship to insulin resistance, glucose intolerance and diabetes mellitus: a review of recent evidence. Drug Saf. 2002;25(3):199-212.
- Nambam B, Schatz D. Growth hormone and insulin-like growth factor-I axis in type 1 diabetes. Growth Horm IGF Res. 2018;38:49-52.
- Attanasio AF, Jung H, Mo D, et al. Prevalence and incidence of diabetes mellitus in adult patients on growth hormone replacement for growth hormone deficiency: a surveillance database analysis. J Clin Endocrinol Metab. 2011;96(7):2255-61.
- Bonfig W, Lindberg A, Carlsson M, et al. Efficacy of Growth Hormone Treatment in Children with Type 1 Diabetes Mellitus and Growth Hormone Deficiency-An Analysis of KIGS Data. J Pediatr. 2018;198:260-264.
- Granado M, García-cáceres C, Tuda M, Frago LM, Chowen JA, Argente J. Insulin and growth hormone-releasing peptide-6 (GHRP-6) have differential beneficial effects on cell turnover in the pituitary, hypothalamus and cerebellum of streptozotocin (STZ)-induced
diabetic rats. Mol Cell Endocrinol. 2011;337(1-2):101-13. - Bailey CJ, Wilkes LC, Flatt PR, Conlon JM, Buchanan KD. Effects of growth hormone-releasing hormone on the secretion of islet hormones and on glucose homeostasis in lean and genetically obese-diabetic (ob/ob) mice and normal rats. J Endocrinol (1989)
123(1):19–24.10.1677/joe.0.1230019. - Ludwig B, Ziegler CG, Schally AV, Richter C, Steffen A, Jabs N, et al. Agonist of growth hormone-releasing hormone as a potential effector for survival and proliferation of pancreatic islets. Proc Natl Acad Sci U S A (2010) 107(28):12623–8.10.1073/pnas.1005098107.
- Ludwig B, Rotem A, Schmid J, Weir GC, Colton CK, Brendel MD, et al. Improvement of islet function in a bioartificial pancreas by enhanced oxygen supply and growth hormone releasing hormone agonist. Proc Natl Acad Sci U S A (2012) 109(13):5022–7.10.1073/pnas.1201868109.
- Zhang X, Cui T, He J, Wang H, Cai R, Popovics P, et al. Beneficial effects of growth hormone-releasing hormone agonists on rat INS-1 cells and on streptozotocin-induced NOD/SCID mice. Proc Natl Acad Sci U S A (2015) 112(44):13651–6.10.1073/pnas.1518540112.
- Schubert U, Schmid J, Lehmann S, Zhang XY, Morawietz H, Block NL, et al. Transplantation of pancreatic islets to adrenal gland is promoted by agonists of growth-hormone-releasing hormone. Proc Natl Acad Sci U S A (2013) 110(6):2288–93.10.1073/pnas.1221505110.
- Schmid J, Ludwig B, Schally AV, Steffen A, Ziegler CG, Block NL, et al. Modulation of pancreatic islets-stress axis by hypothalamic releasing hormones and 11beta-hydroxysteroid dehydrogenase. Proc Natl Acad Sci U S A (2011) 108(33):13722–7.10.1073/pnas.1110965108.
- Svensson J, Jansson JO, Ottosson M, et al. Treatment of obese subjects with the oral growth hormone secretagogue MK-677 affects serum concentrations of several lipoproteins, but not lipoprotein(a). J Clin Endocrinol Metab. 1999;84(6):2028-33.
- Hersch EC, Merriam GR. Growth hormone (GH)–releasing hormone and GH secretagogues in normal aging: Fountain of Youth or Pool of Tantalus? Clinical Interventions in Aging. 2008;3(1):121-129.
- Sigalos JT, Pastuszak AW. The Safety and Efficacy of Growth Hormone Secretagogues. Sex Med Rev. 2018;6(1):45-53.
- O’neal DN, Hew FL, Best JD, Alford F. The effect of 24 months recombinant human growth hormone (rh-GH) on LDL cholesterol, triglyceride-rich lipoproteins and apo [a] in hypopituitary adults previously treated with conventional replacement therapy. Growth Horm IGF Res. 1999;9(3):165-73.
- Leese GP, Wallymahmed M, Vanheyningen C, Tames F, Wieringa G, Macfarlane IA. HDL-cholesterol reductions associated with adult growth hormone replacement. Clin Endocrinol (Oxf). 1998;49(5):673-7.
- Gács G, Romics L. Effect of growth hormone on serum lipoproteins in growth hormone deficiency. Exp Clin Endocrinol. 1987;90(2):227-31.
- Leonsson M, Oscarsson J, Bosaeus I, et al. Growth hormone (GH) therapy in GH-deficient adults influences the response to a dietary load of cholesterol and saturated fat in terms of cholesterol synthesis, but not serum low density lipoprotein cholesterol levels. J Clin Endocrinol Metab. 1999;84(4):1296-303.
- Zhu WF, Tang SJ, Shen Z, Wang YM, Liang L. Growth hormone reverses dyslipidemia in adult offspring after maternal undernutrition. Sci Rep. 2017;7(1):6038.
- Chen M, Gan D, Luo Y, et al. Effect of recombinant human growth hormone therapy on blood lipid and carotid intima-media thickness in children with growth hormone deficiency. Pediatr Res. 2018;83(5):954-960.
- Tonstad S, Sundt E, Ose L, et al. The effect of growth hormone on low-density lipoprotein cholesterol and lipoprotein (a) levels in familial hypercholesterolemia. Metab Clin Exp. 1996;45(11):1415-21.
- Gács G, Romics L. Effect of growth hormone on serum lipoproteins in growth hormone deficiency. Exp Clin Endocrinol. 1987;90(2):227-31.
- Beentjes JA, Van tol A, Sluiter WJ, Dullaart RP. Effect of growth hormone replacement therapy on plasma lecithin:cholesterol acyltransferase and lipid transfer protein activities in growth hormone-deficient adults. J Lipid Res. 2000;41(6):925-32.
- Xu L, Xu C, Yu C, et al. Association between serum growth hormone levels and nonalcoholic fatty liver disease: a cross-sectional study. PLoS ONE. 2012;7(8):e44136.
- Succurro E, Arturi F, Grembiale A, et al. Positive association between plasma IGF1 and high-density lipoprotein cholesterol levels in adult nondiabetic subjects. Eur J Endocrinol. 2010;163(1):75-80.
- Burchardt P, Tabaczewski P, Goździcka-józefiak A, et al. Association between insulin like growth factor-1 and lipoprotein metabolism in stable angina patients on statin therapy: a pilot study. Kardiol Pol. 2012;70(10):1017-22.
- Liang S, Hu Y, Liu C, Qi J, Li G. Low insulin-like growth factor 1 is associated with low high-density lipoprotein cholesterol and metabolic syndrome in Chinese nondiabetic obese children and adolescents: a cross-sectional study. Lipids in Health and Disease. 2016;15:112. doi:10.1186/s12944-016-0275-7.
- Eggert ML, Wallaschofski H, Grotevendt A, et al. Cross-sectional and longitudinal relation of IGF1 and IGF-binding protein 3 with lipid metabolism. Eur J Endocrinol. 2014;171(1):9-19.
- Arturi F, Succurro E, Procopio C, et al. Nonalcoholic fatty liver disease is associated with low circulating levels of insulin-like growth factor-I. J Clin Endocrinol Metab. 2011;96(10):E1640-4.
- Izumi S, Ribeiro-filho FF, Carneiro G, Togeiro SM, Tufik S, Zanella MT. IGF-1 Levels are Inversely Associated With Metabolic Syndrome in Obstructive Sleep Apnea. J Clin Sleep Med. 2016;12(4):487-93.
- Wang WC, Chiu YF, Chung RH, et al. Gene Is Associated With Triglyceride Levels In Subjects With Family History Of Hypertension From The SAPPHIRe And TWB Projects. Int J Med Sci. 2018;15(10):1035-1042.
- Cappel M, Mauger D, Thiboutot D. Correlation between serum levels of insulin-like growth factor 1, dehydroepiandrosterone sulfate, and dihydrotestosterone and acne lesion counts in adult women. ArchDermatol.2005;141(3):333-8.
- Sjögren K, Wallenius K, Liu JL, et al. Liver-derived IGF-I is of importance for normal carbohydrate and lipid metabolism. Diabetes. 2001;50(7):1539-45.
- Dichtel LE, Corey KE, Misdraji J, et al. The Association Between IGF-1 Levels and the Histologic Severity of Nonalcoholic Fatty Liver Disease. Clinical and Translational Gastroenterology. 2017;8(1):e217-. doi:10.1038/ctg.2016.72.
- Romero MJ, Lucas R, Dou H, et al. Role of growth hormone-releasing hormone in dyslipidemia associated with experimental type 1 diabetes. Proc Natl Acad Sci USA. 2016;113(7):1895-900.
Patient Success Stories



What to expect during your consultation:
- Usually takes 15-30 minutes
- Completely confidential
- No obligation to purchase anything
- We will discuss your symptoms along with your health and fitness goals
- Free post-consult access for any additional questions you may have
Free Consultation
Start Your Journey to a Younger, Healthier You!



Subscribe




Free Consultation
STEPS AWAY FROM A YOUNGER. HEALTHIER YOU!
Call 800-277-4041 for a Free Consultation
What to expect during your consultation:
- Usually takes 15-30 minutes
- Completely confidential
- No obligation to purchase anything
- We will discuss your symptoms along with your health and fitness goals
- Free post-consult access for any additional questions you may have