
Potential Benefits of CJC 1295
- Improves muscle mass and strength [1-38]
- Promotes weight loss [39-57]
- Improves sleep quality [58-84]
- Improves cognitive function [85-98]
- Maintains a healthy skeletal frame [99-142]
- Improves mood and energy levels [143-168]
- Improves sex drive and sexual function [169-206]
- Enhances tissue regeneration [207-233]
- Strengthens the immune system [234-260]
- Improves women’s fertility [263]
What is CJC 1295?
CJC-1295 is also known as drug affinity complex: growth hormone-releasing factor (DAC: GRF) or CJC 1295 DAC. It’s a synthetic analogue of growth hormone-releasing hormone (GHRH) and is primarily used to boost blood levels of human growth hormone by up to ten times its normal capacity. CJC-1295 can boost serum growth hormone levels by 200-1000% and the elevated growth hormone production can continue for up to 6 days.
Because CJC-1295 has a similar structure to GHRH, it has the ability to stimulate the pituitary gland to release growth hormone as well as other anabolic hormones such as insulin-like growth factor 1 or insulin growth factor 1. For this reason, many bodybuilders and athletes use CJC-1295 in order to improve muscle mass and strength, as well as performance. Originally, CJC-1295 and other synthetic peptides (compounds consisting of two or more amino acids linked in a chain) were commonly prescribed by medical professionals to treat patients suffering from muscle wasting, growth disorders, and burn injuries. Today, CJC-1295 is still widely prescribed in the treatment of these disorders because of its minimal side effects.
In general, patients who want to reap the potential health benefits of CJC-1295 may need 2 to 3 times daily injections (morning, before sleep, and after a workout). This method of administration is meant to mimic the actual secretion of growth hormones. Additionally, CJC-1295 has a long half-life. A longer half-life means its effects are not affected by food timing like other peptides.
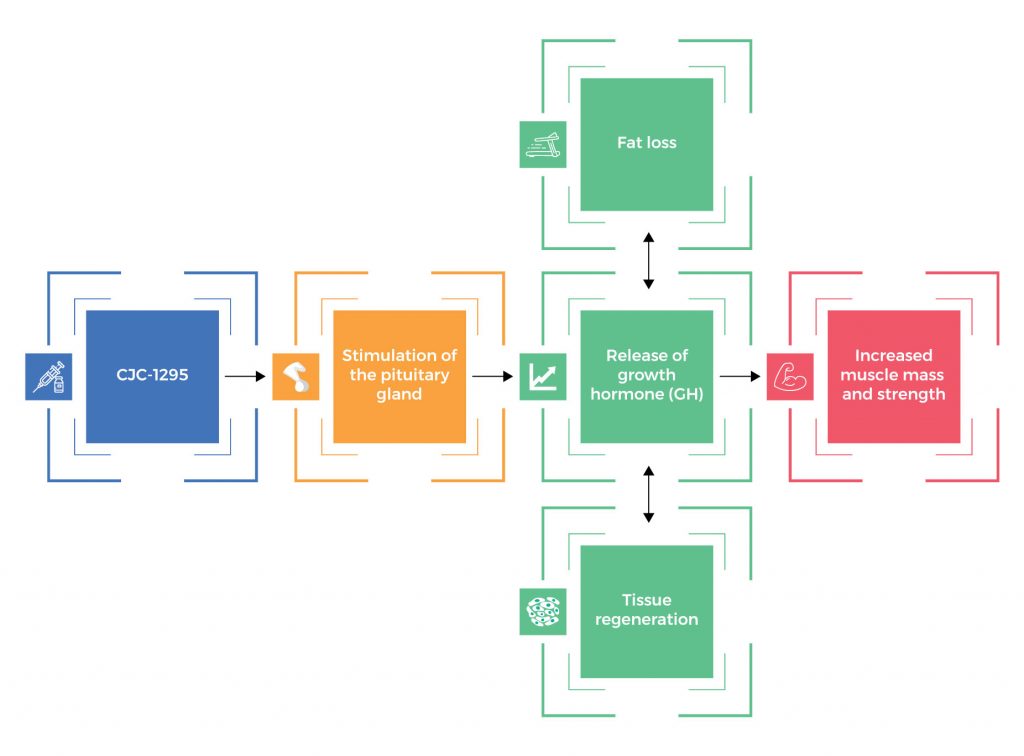
How CJC 1295 Works
CJC-1295 stimulates the pituitary gland to release growth hormone (GH). In order to ensure balance (homeostasis), the human body still releases growth hormone in pulses. With increased GH levels, it leads to increased muscle mass and strength, fat loss, tissue regeneration, and other health benefits.
Chemical Structure of CJC 1295
Research on CJC 1295 Benefits
A. Improves Muscle Mass and Strength

CJC-1295 is a peptide known for its ability to increase muscle mass and strength by stimulating the release of growth hormone (GH) from the pituitary gland. This synthetic peptide enhances the pulsatile release of GH, which in turn promotes protein synthesis, muscle growth, and repair, making it a valuable tool for building muscle. Increased GH levels can lead to more efficient utilization of nutrients and improved muscle recovery, ultimately contributing to more muscle mass and enhanced muscle strength over time. Interestingly, an increase in muscle mass boosts allows the body’s resting metabolic rate to be boosted leading to more calories burned.
Studies show that this powerful peptide can boost the production of muscle cells:
- In normal adult subjects, CJC-1295 administration enhanced muscle mass and strength by increasing protein synthesis. [1]
- In healthy adult participants, subcutaneous administration of CJC-1295 safely and effectively increased plasma GH concentrations and IGF-1 levels, resulting in an increase in muscle mass and strength.[2]
- By increasing GH and IGF-1 levels, CJC-1295 significantly improved muscle mass and strength in both men and women subjects. [3-36]
- In mice, treatment with once-daily administration of CJC-1295 maintained normal body composition as well as muscle mass. [37-38]
B. Promotes Weight Loss

CJC-1295 promotes weight loss by stimulating the release of growth hormone from the pituitary gland, which in turn enhances the body’s ability to metabolize fat and build lean muscle tissue. This increase in growth hormone levels can lead to a higher metabolism, improved fat oxidation, and reduced body fat storage, ultimately contributing to weight loss and body composition improvements when combined with a healthy diet and exercise regimen.
Studies show that CJC-1295 can promote weight loss by burning more body fat and increasing lean muscle mass:
- In obese patients, CJC-1295 promoted fat loss by increasing the levels of growth hormone. [39-42]
- In healthy adults, subcutaneous administration of CJC-1295 safely and effectively increased GH and IGF-1 levels, resulting in a significant reduction in body fat percentage and body mass index (BMI). [43]
- In women, the use of synthetic growth hormone CJC-1295 reduced body weight. [44]
- In both men and women, CJC-1295 reduced body weight by boosting growth hormone levels. [45-56]
- In mice, treatment with once-daily administration of CJC-1295 improved body composition by preventing fat accumulation. [57]
C. Improves Sleep Quality

CJC-1295 can potentially improve sleep quality by stimulating the release of growth hormone (GH) during deep sleep stages. This peptide increases GH secretion, which is essential for restorative sleep, tissue repair, and overall sleep quality, offering a tremendous benefit. Improved sleep patterns and deeper sleep can contribute to a more refreshing and restful night’s sleep when CJC-1295 is used as part of a well-balanced peptide therapy under medical supervision.
Studies show that this powerful peptide can help you get a restful sleep:
- A study reported that CJC-1295 can improve sleep quality and quantity by promoting slow wave sleep, also known as the deep sleep stage. [58]
- In mice, once-daily administration of CJC-1295 normalized the GHRH response, which in turn induced significantly deeper sleep. [59]
- Studies found that by increasing GH levels, CJC-1295 can significantly improve the deep sleep stage. [60-65]
- In patients with insomnia, the administration of delta sleep-inducing peptides such as CJC-1295 was associated with higher sleep efficiency and shorter sleep latency (amount of time it takes to fall asleep). [66]
- In men, the administration of GHRH such as CJC-1295 promoted deep sleep by enhancing stage 2 sleep. [67]
- In normal men, the administration of GHRH such as CJC-1295 was associated with a 10-fold increase in slow wave sleep. [68]
- As a growth hormone-releasing factor, CJC-1295 induces sleep by activating sleep regulatory neurons in the brain. [69-70]
- In patients with schizophrenia, a chronic and severe mental disorder that alters cognition, emotion, and behavior, the administration of GHRH such as CJC-1295 improved sleep efficiency. [71]
- Studies showed that CJC-1295 can increase non-rapid eye movement (NREM) sleep and enhance EEG slow-wave activity (SWA). [72-83]
- In rats, the injection of GHRH such as CJC-1295 effectively promoted sleep. [84]
D. Improves Cognitive Function

CJC-1295, a very effective peptide and a growth hormone-releasing hormone (GHRH) analog, is believed to potentially treat diseases and enhance cognition and memory function by promoting the release of growth hormone in the body. Growth hormone plays a role in neurogenesis (the formation of new neurons), neuronal survival, and synaptic plasticity, all of which are essential for optimal brain function. By increasing growth hormone levels, CJC-1295 may support improved cognitive processes such as memory, learning, feeling mental clarity, and overall brain health, leading to a significant difference in the improved overall benefit for individuals seeking enhanced cognitive function.
There is increasing scientific evidence that GHRH like CJC-1295 can help combat cognitive impairment associated with advancing age and other medical conditions:
- In adults with mild cognitive impairment and healthy older adults, GHRH treatment significantly improved verbal memory. [85]
- In healthy older adults, GHRH supplementation ameliorated cognitive impairment associated with aging and Alzheimer’s disease. [86]
- In adults with mild cognitive impairment, GHRH supplementation improved cognitive function by boosting the levels of brain chemicals such as Gamma-Aminobutyric acid (GABA) and N-acetylaspartylglutamate (NAAG). [87]
- In older adults, GHRH supplementation improved various aspects of cognitive function. [88]
- In adults with mild cognitive impairment, GHRH supplementation slowed cognitive decline. [89-90]
- Studies reported that CJC-1295 improves cognitive function through its neuroprotective effects, allowing it to prevent damage to nerve cells in the brain. [91-92]
- In adults who are at increased risk of cognitive decline and dementia, GHRH administration had favorable effects on cognitive function. [93]
- In rats with traumatic brain injury, GHRH administration appears to improve cognitive function. [94-98]
E. Maintains a Healthy Skeletal Frame

Strong scientific evidence suggests that CJC-1295 plays an integral part in the maintenance of bone health and the prevention of bone disorders, such as osteoporosis and fractures, by stimulating the production of growth hormone, which in turn can enhance increased bone density and promote bone remodeling processes:
- In men with HIV-related fat accumulation, GHRH administration improved bone metabolism and bone density, suggesting that CJC-1295 can correct various bone disorders. [99]
- In elderly postmenopausal women with decreased bone mass, treatment with GHRH stimulated bone metabolism. [100]
- In healthy elderly women, GHRH administration prevented bone breakdown by increasing the blood levels of bone formation markers. [101]
- In patients with primary and secondary osteoporosis, GHRH administration increased bone formation and activity of bone cells (osteoblasts). [102]
- In women with postmenopausal osteoporosis, GHRH administration accelerated bone metabolism and activity of osteoblasts. [103-113]
- In men with osteoporosis of unknown cause, boosting GH levels through GHRH administration significantly improved bone mineral density (BMD). [114-115]
- In GH-deficient adults with osteoporosis, GHRH administration increased BMD and markers of bone formation and decreased markers of bone breakdown. [116-118]
- In patients with fractures, GHRH administration accelerated fracture healing. [119]
- In mice, CJC-1295 administration helped normalize bone growth in the legs. [120]
- Studies found that by increasing GH levels, CJC-1295 can significantly lower one’s risk of osteoporosis, fractures, and other bone disorders. [121-142]
F. Improves Mood and Energy Levels

Because of CJC-1295’s ability to boost GH levels by up to ten times its normal capacity, it can also help improve mood and energy levels in people suffering from depression, anxiety, and other mood disorders. There is compelling evidence supporting the beneficial effects of CJC-1295 on mood:
- Several studies showed that low blood levels of growth hormone were strongly linked with depression, anxiety, and other mood disorders, suggesting that the administration of GHRH such as CJC-1295 may help improve mood and energy levels by boosting GH production in the body. [143-156]
- In adults with mild cognitive impairment and healthy older adults, GHRH administration had favorable effects on cognition and mood. [157]
- In patients with major depression, GHRH administration increased GH levels, resulting in a reduction of depressive symptoms. [158]
- In patients with major depression, GHRH administration improved energy levels by decreasing sleepiness. [159]
- In patients with depression, GHRH administration significantly improved mood and energy levels by increasing the levels of neurotransmitters (brain chemicals) such as noradrenaline, dopamine, and acetylcholine. [160-168]
G. Improves Sex Drive and Sexual Function

Because CJC-1295 has a similar structure to GHRH, it can stimulate the pituitary gland to release various hormones that are involved in the regulation of sex drive and the ability to function properly sexually. Studies show that by boosting the levels of anabolic hormones such as growth hormone and insulin-like growth factor 1 (IGF-1), CJC 1295 may help ramp up sexual power and fight sexual dysfunction:
- Studies showed that growth hormone deficiency was strongly linked with low libido and erectile dysfunction, suggesting that increasing GH levels through CJC-1295 supplementation may have beneficial effects on sex drive and sexual function. [169-176]
- Studies also showed that IGF-1 deficiency was strongly linked with low libido and erectile dysfunction, suggesting that CJC-1295 supplementation may help improve sexual function. [177-183]
- In age-advanced men, GHRH supplementation significantly improved libido and general well-being. [184]
- Studies have shown that by increasing GH and IGF-1 levels, CJC-1295 also increases the levels of nitric oxide, a molecule naturally produced in the body which plays an integral part in penile erection. [185-193]
- Studies found that CJC-1295 administration improved sex drive and sexual function by increasing GH levels, which in turn boosts the levels of the primary male sex hormone testosterone and the primary female sex hormone estrogen. [194-195]
- Studies showed that peptides such as CJC-1295 were involved in the erection process and sexual arousal. [196-205]
- In animal models, GHRH administration increased testicular responsiveness and receptors. [206]
H. Enhances Tissue Regeneration

CJC-1295 can indirectly improve tissue regeneration of almost all body systems. Studies show that by stimulating the pituitary gland to release two vital hormones, GH and IGF-1, CJC-1295 may accelerate tissue repair after an injury:
- In the human tendon and skeletal muscle, GH repaired the damaged tissues by stimulating collagen synthesis. [207]
- A study reported that IGF-1 has a potential role in enhancing stem cell repair after a kidney injury. [208]
- A number of studies found that both GH and IGF-1 may play a role in brain repair after an injury. [209-218]
- Studies also showed that both GH and IGF-1 may help accelerate tissue repair by increasing collagen synthesis. [219-220]
- As a GHRH, CJC-1295 has been found to accelerate the wound healing process by promoting the formation of a protective covering of damaged skin tissues. [221-223]
- Recent evidence showed that CJC-1295 and other GHRHs can induce heart repair after myocardial infarction by mechanisms involving a direct action on the heart cells (cardiomyocytes). [224-225]
- A cell study found that GHRH promoted tissue regeneration by stimulating the proliferation of the cells of the pancreas while preventing programmed cell death (apoptosis). [226]
- Numerous studies found that GHRH administration accelerated the repair of tissue injury by increasing the number of cells needed for regeneration at the site of injury, suggesting that it may be a potential treatment for acute musculoskeletal injuries. [227-232]
- GHRH administration can also help improve the healing of debilitating injuries such as Achilles tendon rupture. [233]
I. Strengthens the Immune System
CJC-1295 can potentially contribute to a strong immune system by stimulating the production and release of growth hormone, which plays a vital role in supporting immune function. As a GHRH, CJC-1295 also possesses immune-modulating properties necessary for a strong immune system:
- In older men and women with compromised immune function, GHRH administration had profound immune-enhancing effects as evidenced by an increase in B and T cells of the immune system. [234]
- In animal models, GHRH injection increased the numbers of CD2, T-cells, and CD4 cells of the immune system. [235-237]
- Evidence suggests that GHRHs such as CJC-1295 strengthen the immune system by regulating the activities of natural killer cells and T cells. [238-241]
- In animal models, GHRH administration for 6 months increased the production of antibodies. [242]
- By increasing GH levels, CJC-1295 improved various aspects of the immune function in both human and animal subjects. [243-246]
- By boosting the levels of IGF-1, CJC-1295 also helps regulate immune function. [247-256]
- GHRH administration can also help fight inflammatory diseases by significantly reducing the levels of inflammatory substances in the body. [257-259]
- GHRH also has the ability to prevent the progression of tumors. [260]
J. Improves Women’s Fertility
There are also studies linking insulin-like growth factor-1 (IGF-1) and growth hormone to improved fertility in women:
- Strong scientific evidence suggests that insulin-like growth factor-1 (IGF-1) and growth hormone can improve fertility by regulating the ovarian follicular cycle. [261-262]
- A cell study investigated the effects of growth hormone releasing factor (GRF) on the ovulation cycle and found that cells treated with GRF had a significant increase in both follicular fluid IGF-1 levels and blood levels of GH, which in turn induced superovulation. [263]
CJC-1295 and Human Growth Hormone
CJC-1295 is a synthetic peptide that has garnered attention in the world of health and fitness due to its potential effects on growth hormone (GH) secretion. It is designed to mimic the action of the natural hormone growth hormone-releasing hormone (GHRH). GHRH stimulates the pituitary gland to produce growth hormone and release it into the bloodstream. CJC-1295, when administered, extends the half-life of GHRH in the body, making it more effective at stimulating the secretion of GH.
CJC-1295 and the Benefits of Elevated Growth Hormone Production
CJC-1295 is a synthetic peptide that mimics the action of GHRH, which stimulates the pituitary gland to produce growth hormone. When used responsibly and under medical supervision, CJC-1295 peptide therapy can offer several potential benefits associated with elevated GH production:
- Muscle growth and repair
- Fat loss
- Enhanced bone density
- Anti-aging effects (e.g. improved skin elasticity)
- Improved sleep and recovery
- Increased energy levels
- Enhanced immune function
- Connective tissue repair
- Mood and cognitive function
CJC 1295 Side Effects
CJC-1295 side effects are very uncommon and generally mild. There have been some side effects associated with the use of this drug wherein the patient had one of the issues listed below at some point while being on CJC-1295. However, these side effects weren’t confirmed to be associated with the treatment and could have been a coincidence and not related to the use of CJC-1295. Despite this, it was listed as a side effect associated with CJC-1295 even though these associated side effects are very uncommon.
Side effects associated with CJC-1295 may include the following:
- Difficulty swallowing
- Dizziness
- Drowsiness
- Flu-like symptoms
- Flushing of the skin
- Headache
- Hives or rashes
- Hyperactivity
- Injection site reactions (irritation, redness, pain, or itching)
- Nausea
CJC 1295 Dosage
The dosage of CJC-1295 can vary depending on the individual’s needs and goals. However, a typical starting dose for adults is 100-200 mcg (micrograms) administered via subcutaneous injection (just beneath the skin) once daily. The dosage can be adjusted up or down as needed.
CJC 1295 Price
The price of CJC-1295, a synthetic peptide used in the field of research and development, can vary depending on several factors such as the supplier, the quantity you’re purchasing, the purity of the product, and your location. Additionally, prices can change over time due to market fluctuations and changes in supply and demand.
The Power of CJC 1295 and Ipamorelin Combination
CJC-1295 and Ipamorelin are typically combined in peptide therapy due to their known compatibility and synergy. When combined, CJC 1295 and Ipamorelin can create a synergistic effect, amplifying their respective abilities to stimulate increased growth hormone secretion. This synergy is achieved by addressing two critical aspects of GH release:
- Increased Pulse Frequency: CJC 1295’s rapid onset extends the duration of GH-releasing hormone activity in the body, leading to more frequent GH pulses. These frequent pulses mimic the body’s natural GH release pattern during youth.
- Amplified GH Release: Ipamorelin, on the other hand, enhances the magnitude of GH release. By acting on pituitary receptors, it promotes a robust surge of GH, contributing to the overall elevations in GH levels.
CJC-1295 takes anywhere from 1-4 hours to reach peak serum levels in the blood, while Ipamorelin works much quicker. Ipamorelin is cleared from the body more rapidly with a half-life of about 2 hours. The combination of both peptides ensures a rapid onset with Ipamorelin and lasting effects with CJC-1295. Because of this, CJC 1295 and Ipamorelin are often incorporated into hormone replacement therapy regimens to stimulate natural growth hormone production and counter the effects of hormonal imbalances.
CJC 1295 Ipamorelin Before and After
CJC 1295-Ipamorelin combination is used for various purposes, including increasing muscle mass, fat loss, and anti-aging effects. In addition, CJC 1295 and Ipamorelin are commonly included in hormone replacement therapy regimens to optimize hormone levels and promote overall well-being. Moreover, ipamorelin improves insulin sensitivity, thus reducing high blood sugars in diabetic patients and the body’s triglycerides. However, it’s important to note that the effects of these peptides can vary from person to person, and results may not be as dramatic as with other substances like anabolic steroids. Additionally, the use of CJC 1295-Ipamorelin combination should be conducted under the guidance of a qualified healthcare professional and in compliance with all relevant laws and regulations.
About Dr. George Shanlikian
Dr. George Shanlikian, renowned as the world’s best hormone therapy doctor, possesses expertise in various medical domains. These include Bio-Identical Hormone Replacement Therapy, Peptide Replacement Therapy, Anti-Aging Medicine, Regenerative Medicine, Stress Management, Nutrition Consulting, Nutritional Supplement Consulting, and Exercise Consulting.
Read more about him here: https://www.genemedics.com/dr-george-shanlikian-md-best-hormone-therapy-doctor
Read more success stories here:
Men’s Success Stories: https://www.genemedics.com/about-ghi/ghi-success-stories/mens-success-stories/
Women’s Success Stories: https://www.genemedics.com/about-ghi/ghi-success-stories/womens-success-stories/
CJC 1295 Ipamorelin Dosage
CJC 1295-Ipamorelin dosage can vary depending on the individual’s needs and goals. However, a typical starting dose for adults is 100-200 mcg (micrograms) of each peptide subcutaneously (under the skin) once daily. The dosage can be adjusted up or down as needed.
CJC-1295 is a long-acting growth hormone secretagogue, which means that it stimulates the release of growth hormone from the pituitary gland. Ipamorelin is a ghrelin receptor agonist, which means that it mimics the effect of the hormone ghrelin, which is responsible for stimulating appetite and growth hormone release.
CJC 1295-Ipamorelin combination has been shown to be more effective at increasing growth hormone levels than either peptide alone. It is also thought to be safer than other growth hormone-releasing peptides, such as GHRP-6 and GHRP-2, which can have side effects such as headaches and nausea.
Here are some additional things to keep in mind about CJC 1295-Ipamorelin dosage:
- The dosage may need to be adjusted based on the individual’s response.
- It is important to inject CJC-1295 and Ipamorelin at the same time each day.
- CJC 1295-Ipamorelin combination should not be used or taken together with other growth hormone secretagogues or growth hormone supplements.
- CJC 1295-Ipamorelin combination should not be taken by pregnant or breastfeeding women.
If you are considering taking CJC 1295-Ipamorelin to attain optimal health, it is important to do your research and talk to a doctor to make sure it is right for you.
FAQ
How many times a week should I take CJC-1295?
Most people take CJC-1295 once a day.
How long does it take for CJC-1295 to work?
It can take 2-4 weeks to see results from CJC-1295.
What are the long term benefits of CJC-1295?
It can help increase muscle mass, strength, and bone density. It can also help improve skin health, improve sleep quality, enhance insulin sensitivity, increase energy levels, and reduce wrinkles.
How long after injecting CJC-1295 can you eat?
You can eat immediately after injecting CJC-1295.
How long can you stay on CJC-1295 Ipamorelin?
It is generally recommended to stay on CJC-1295 Ipamorelin for 12-24 weeks.
Does CJC-1295 increase muscle mass?
Yes, CJC-1295 can help increase muscle mass.
Does CJC-1295 make you hungry?
CJC-1295 can make you feel hungry, but this is not a universal side effect.
Does CJC-1295 increase collagen?
Yes, CJC-1295 can help increase collagen production.
Does CJC-1295 burn fat?
CJC-1295 can help burn fat, but this is not its primary function.
How long does CJC-1295 stay in your system?
CJC-1295 has a half-life of 36 hours, meaning it takes 36 hours for half of the dose to be eliminated from the body.
Does CJC-1295 really work?
Yes, CJC-1295 has been shown to be effective in increasing muscle mass, strength, and bone density.
How much CJC-1295 should I take a day?
The dosage of CJC-1295 depends on the individual and their goals. A typical dosage is 1-2 mg per day.
What does CJC-1295 feel like?
Most people do not feel any effects from CJC-1295.
Does CJC-1295 help with sleep?
CJC-1295 can help improve sleep quality.
How long does CJC-1295 last?
CJC-1295 can last for up to 36 hours.
Can you take CJC-1295 on an empty stomach?
It is best to take CJC-1295 on an empty stomach.
What is the best combination with CJC 1295?
The best combination with CJC-1295 is Ipamorelin.
Why take CJC-1295 at night?
CJC-1295 can help improve sleep quality, so it is often taken at night.
How long does it take to see results from CJC-1295 Ipamorelin?
It can take 2-4 weeks to see results from CJC-1295 Ipamorelin.
Is CJC-1295 natural?
CJC-1295 is not a natural substance. It is a synthetic peptide that is designed to mimic the effects of growth hormone.
Does CJC-1295 increase cortisol?
CJC-1295 does not increase cortisol levels.
Does CJC 1295 affect testosterone?
CJC-1295 typically does not directly affect testosterone levels as its primary action is related to stimulating the release of growth hormone, but it may have indirect effects on testosterone through its influence on hormonal balance.
Reference
Sackmann-Sala L, Ding J, Frohman LA, Kopchick JJ. Activation of the GH/IGF-1 axis by CJC-1295, a long acting GHRH analog, results in serum protein profile changes in normal adult subjects. Growth hormone & IGF research : official journal of the Growth Hormone Research Society and the International IGF Research Society. 2009;19(6):471-477. doi:10.1016/j.ghir.2009.03.001.
Teichman SL, Neale A, Lawrence B, Gagnon C, Castaigne JP, Frohman LA. Prolonged stimulation of growth hormone (GH) and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults. J Clin Endocrinol Metab. 2006;91(3):799-805.
Tavares ABW, Micmacher E, Biesek S, et al. Effects of Growth Hormone Administration on Muscle Strength in Men over 50 Years Old. International Journal of Endocrinology. 2013;2013:942030. doi:10.1155/2013/942030.
Taaffe DR, Pruitt L, Reim J, et al. Effect of recombinant human growth hormone on the muscle strength response to resistance exercise in elderly men. J Clin Endocrinol Metab. 1994;79(5):1361-6.
Sattler FR, Castaneda-Sceppa C, Binder EF, et al. Testosterone and Growth Hormone Improve Body Composition and Muscle Performance in Older Men. The Journal of Clinical Endocrinology and Metabolism. 2009;94(6):1991-2001. doi:10.1210/jc.2008-2338.
Rennie M. Claims for the anabolic effects of growth hormone: a case of the Emperor’s new clothes? British Journal of Sports Medicine. 2003;37(2):100-105. doi:10.1136/bjsm.37.2.100.
Velloso CP. Regulation of muscle mass by growth hormone and IGF-I. British Journal of Pharmacology. 2008;154(3):557-568. doi:10.1038/bjp.2008.153.
Adams GR. Insulin-like growth factor in muscle growth and its potential abuse by athletes. Western Journal of Medicine. 2001;175(1):7-9.
Welle S, Thornton C, Statt M, Mchenry B. Growth hormone increases muscle mass and strength but does not rejuvenate myofibrillar protein synthesis in healthy subjects over 60 years old. J Clin Endocrinol Metab. 1996;81(9):3239-43.
Harman SM, Blackman MR. The effects of growth hormone and sex steroid on lean body mass, fat mass, muscle strength, cardiovascular endurance and adverse events in healthy elderly women and men. Horm Res. 2003;60(Suppl 1):121-4.
Brill KT, Weltman AL, Gentili A, et al. Single and combined effects of growth hormone and testosterone administration on measures of body composition, physical performance, mood, sexual function, bone turnover, and muscle gene expression in healthy older men. J Clin Endocrinol Metab. 2002;87(12):5649-57.
Brill KT, Weltman AL, Gentili A, et al. Single and combined effects of growth hormone and testosterone administration on measures of body composition, physical performance, mood, sexual function, bone turnover, and muscle gene expression in healthy older men. J Clin Endocrinol Metab. 2002;87(12):5649-57.
Molitch ME, Clemmons DR, Malozowski S, Merriam GR, Vance ML. Evaluation and treatment of adult growth hormone deficiency: an endocrine society clinical practice guideline. Journal of Clinical Endocrinology and Metabolism. 2011;96(6):1587–1609.
Lanfranco R, Pellegrino M, Maccario M, Arvat E. Ageing, growth hormone and physical performance. Journal of Endocrinological Investigation. 2003;26(9):861–872.
Lange KHW, Andersen JL, Beyer N, et al. GH administration changes myosin heavy chain isoforms in skeletal muscle but does not augment muscle strength or hypertrophy, either alone or combined with resistance exercise training in healthy elderly men. Journal of Clinical Endocrinology and Metabolism. 2002;87(2):513–523.
Taaffe DR, Pruitt L, Reim J, et al. Effect of recombinant human growth hormone on the muscle strength response to resistance exercise in elderly men. Journal of Clinical Endocrinology and Metabolism. 1994;79(5):1361–1366.
Papadakis MA, Grady D, Black D, et al. Growth hormone replacement in healthy older men improves body composition but not functional ability. Annals of Internal Medicine. 1996;124(8):708–716.
Yarasheski KE, Zachwieja JJ, Campbell JA, Bier DM. Effect of growth hormone and resistance exercise on muscle growth and strength in older men. American Journal of Physiology-Endocrinology and Metabolism. 1995;268(2):E268–E276.
Weltman A, Weltman JY, Schurrer R, Evans WS, Veldhuis JD, Rogol AD. Endurance training amplifies the pulsatile release of growth hormone: effects of training intensity. Journal of Applied Physiology. 1992;72(6):2188–2196.
Poehlman ET, Copeland KC. Influence of physical activity on insulin-like growth factor-I in healthy younger and older men. Journal of Clinical Endocrinology and Metabolism. 1990;71(6):1468–1473.
Blackman MR, Sorkin JD, Munzer T, Bellantoni MF, Busby-Whitehead J, Stevens TE, Jayme J, O’Connor KG, Christmas C, Tobin JD, Stewart KJ, Cottrell E, St. Clair C, Pabst KM, Harman SM 2002 Growth hormone and sex steroid administration in healthy aged women and men: a randomized controlled trial. JAMA 288:2282–2292.
Brill KT, Weltman AL, Gentili A, Patrie JT, Fryburg DA, Hanks JB, Urban RJ, Veldhuis JD 2002 Single and combined effects of growth hormone and testosterone administration on measures of body composition, physical performance, mood, sexual function, bone turnover, and muscle gene expression in healthy older men. J Clin Endocrinol Metab 87:5649–5657.
Rudman D, Feller AG, Nagraj HS, Gergans GA, Lalitha PY, Goldberg AF, Schlenker RA, Cohn L, Rudman IW, Mattson DE 1990 Effects of human growth hormone in men over 60 years old. N Engl J Med 323:1–6.
Welle S, Thornton C, Statt M, McHenry B 1996 Growth hormone increases muscle mass and strength but does not rejuvenate myofibrillar protein synthesis in healthy subjects over 60 years old. J Clin Endocrinol Metab 81:3239–3243.
Papadakis MA, Grady D, Black D, Tierney MJ, Gooding GA, Schambelan M, Grunfeld C 1996 Growth hormone replacement in healthy older men improves body composition but not functional ability [see comments]. Ann Intern Med 124:708–716.
Lange KH, Larsson B, Flyvbjerg A, Dall R, Bennekou M, Rasmussen MH, Orskov H, Kjaer M 2002 Acute growth hormone administration causes exaggerated increases in plasma lactate and glycerol during moderate to high intensity bicycling in trained young men. J Clin Endocrinol Metab 87:4966–4975.
Hennessey JV, Chromiak JA, DellaVentura S, Reinert SE, Puhl J, Kiel DP, Rosen CJ, Vandenburgh H, MacLean DB 2001 Growth hormone administration and exercise effects on muscle fiber type and diameter in moderately frail older people. J Am Geriatr Soc 49:852–858.
Taaffe DR, Pruitt L, Reim J, Hintz RL, Butterfield G, Hoffman AR, Marcus R 1994 Effect of recombinant human growth hormone on the muscle strength response to resistance exercise in elderly men. J Clin Endocrinol Metab 79:1361–1366.
Yarasheski KE, Zachwieja JJ, Campbell JA, Bier DM 1995 Effect of growth hormone and resistance exercise on muscle growth and strength in older men. Am J Physiol 268:E268–E276.
D’Ercole J, Stiles AD, Underwood LE. Tissue concentrations of somatomedin C: further evidence for multiple sites of synthesis and paracrine or autocrine mechanisms of action. Proc Natl Acad Sci USA. 1984;81:935–939.
Gostelli-Peter M, Winterhalter KH, Schmid C, Froesch ER, Zapf J. Expression and regulation of insulin like growth factor I (IGF-I) and IGF binding protein messenger ribonucleic acid levels in tissues of hypophysectomized rats infused with IGF-I and growth hormone. Endocrinology. 1994;135:2558–2567.
Smit LS, Meyer DJ, Billestrup N, Norstedt G, Schwartz J, Carter-Su C. The role of the growth hormone (GH) receptor and JAK1 and JAK2 kinases in the activation of Stats 1, 3, and 5 by GH. Mol Endocrinol. 1996;10:519–533.
Adams GR. The role of IGF-I in the regulation of skeletal muscle adaptation. Exerc Sport Sci Rev 1998;26: 31-60.
Taaffe DR, Jin IH, Vu TH, et al. Lack of effect of recombinant human growth hormone (GH) on muscle morphology and GH-insulin-like growth factor expression. J Clin Endocrinol Metab 1996;81: 421-425.
Taaffe DR, Pruitt L, Reim J, et al. Effect of recombinant human growth hormone on the muscle strength response to resistance exercise in elderly men. J Clin Endocrinol Metab 1994;79: 1361-1366.
Yarasheski KE, Zachwieja JJ, Campbell JA, et al. Effect of growth hormone and resistance exercise on muscle growth and strength in older men. Am J Physiol 1995;268: E268-E276.
Alba M, Fintini D, Sagazio A, et al. Once-daily administration of CJC-1295, a long-acting growth hormone-releasing hormone (GHRH) analog, normalizes growth in the GHRH knockout mouse. Am J Physiol Endocrinol Metab. 2006;291(6):E1290-4.
Gautam D, Jeon J, Starost MF, et al. Neuronal M3 muscarinic acetylcholine receptors are essential for somatotroph proliferation and normal somatic growth. Proc Natl Acad Sci USA. 2009;106(15):6398-403.
Engelson ES, Glesby MJ, Mendez D, Albu JB, Wang J, Heymsfield SB, Kotler DP 2002 Effect of recombinant human growth hormone in the treatment of visceral fat accumulation in HIV infection. J Acquired Immune Defic Syndr 30:379–391.
Falutz J, Allas S, Kotler D, Thompson M, Koutkia P, Albu J, Trottier B, Routy J-P, Cote P, Abribat T, Grinspoon S 2005 A placebo-controlled, dose-ranging study of a growth hormone releasing factor in HIV-infected patients with abdominal fat accumulation. AIDS 19:1279–1287.
Teichman, Sam L.; Neale, Ann; Lawrence, Betty; Gagnon, Catherine; Castaigne, Jean-Paul; Frohman, Lawrence A. (2006). “Prolonged Stimulation of Growth Hormone (GH) and Insulin-Like Growth Factor I Secretion by CJC-1295, a Long-Acting Analog of GH-Releasing Hormone, in Healthy Adults”. The Journal of Clinical Endocrinology & Metabolism. 91 (3): 799–805. doi:10.1210/jc.2005-1536. ISSN 0021-972X. PMID 16352683.
Ionescu, Madalina; Frohman, Lawrence A. (2006). “Pulsatile Secretion of Growth Hormone (GH) Persists during Continuous Stimulation by CJC-1295, a Long-Acting GH-Releasing Hormone Analog”. The Journal of Clinical Endocrinology & Metabolism. 91 (12): 4792–4797. doi:10.1210/jc.2006-1702. ISSN 0021-972X.
Teichman SL, Neale A, Lawrence B, Gagnon C, Castaigne JP, Frohman LA. Prolonged stimulation of growth hormone (GH) and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults. J Clin Endocrinol Metab. 2006;91(3):799-805.
Van hout MC, Hearne E. Netnography of Female Use of the Synthetic Growth Hormone CJC-1295: Pulses and Potions. Subst Use Misuse. 2016;51(1):73-84.
Rasmussen MH. Obesity, growth hormone and weight loss. Mol Cell Endocrinol. 2010;316(2):147-53.
Gertner JM. Effects of growth hormone on body fat in adults. Horm Res. 1993;40(1-3):10-5.
Shadid S, Jensen MD. Effects of growth hormone administration in human obesity. Obes Res. 2003;11(2):170-5.
Kim KR, Nam SY, Song YD, Lim SK, Lee HC, Huh KB. Low-dose growth hormone treatment with diet restriction accelerates body fat loss, exerts anabolic effect and improves growth hormone secretory dysfunction in obese adults. Horm Res. 1999;51(2):78-84.
Thompson JL, Butterfield GE, Gylfadottir UK, et al. Effects of human growth hormone, insulin-like growth factor I, and diet and exercise on body composition of obese postmenopausal women. J Clin Endocrinol Metab. 1998;83(5):1477-84.
Devesa J, Almengló C, Devesa P. Multiple Effects of Growth Hormone in the Body: Is it Really the Hormone for Growth? Clinical Medicine Insights Endocrinology and Diabetes. 2016;9:47-71. doi:10.4137/CMED.S38201.
Skaggs SR, Crist DM. Exogenous human growth hormone reduces body fat in obese women. Horm Res. 1991;35(1):19-24.
Chaves VE, Júnior FM, Bertolini GL. The metabolic effects of growth hormone in adipose tissue. Endocrine. 2013;44(2):293-302.
Mekala KC, Tritos NA. Effects of recombinant human growth hormone therapy in obesity in adults: a meta analysis. J Clin Endocrinol Metab. 2009;94(1):130-7.
Marcovecchio ML, Chiarelli F. Obesity and growth during childhood and puberty. World Rev Nutr Diet. 2013;106:135–141.
De Leonibus C, Marcovecchio ML, Chiarelli F. Update on statural growth and pubertal development in obese children. Pediatr Rep. 2012;4:e35.
Louvi A, Accili D, Efstratiadis A. Growth-promoting interaction of IGF-II with the insulin receptor during mouse embryonic development. Dev Biol. 1997;189:33–48.
Alba M, Fintini D, Sagazio A, et al. Once-daily administration of CJC-1295, a long-acting growth hormone-releasing hormone (GHRH) analog, normalizes growth in the GHRH knockout mouse. Am J Physiol Endocrinol Metab. 2006;291(6):E1290-4.
Teichman SL, Neale A, Lawrence B, Gagnon C, Castaigne JP, Frohman LA. Prolonged stimulation of growth hormone (GH) and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults. J Clin Endocrinol Metab. 2006;91(3):799-805.
Alba M, Fintini D, Sagazio A, et al. Once-daily administration of CJC-1295, a long-acting growth hormone-releasing hormone (GHRH) analog, normalizes growth in the GHRH knockout mouse. Am J Physiol Endocrinol Metab. 2006;291(6):E1290-4.
Morselli LL, Nedeltcheva A, Leproult R, et al. Impact of growth hormone replacement therapy on sleep in adult patients with growth hormone deficiency of pituitary origin. European journal of endocrinology/European Federation of Endocrine Societies. 2013;168(5):10.1530/EJE-12-1037. doi:10.1530/EJE-12-1037.
Haqq AM, Stadler DD, Jackson RH, Rosenfeld RG, Purnell JQ, Lafranchi SH. Effects of growth hormone on pulmonary function, sleep quality, behavior, cognition, growth velocity, body composition, and resting energy expenditure in Prader-Willi syndrome. J Clin Endocrinol Metab. 2003;88(5):2206-12.
Van cauter E, Copinschi G. Interrelationships between growth hormone and sleep. Growth Horm IGF Res. 2000;10 Suppl B:S57-62.
Copinschi G, Nedeltcheva A, Leproult R, et al. Sleep disturbances, daytime sleepiness, and quality of life in adults with growth hormone deficiency. J Clin Endocrinol Metab. 2010;95(5):2195-202.
Davidson JR, Moldofsky H, Lue FA. Growth hormone and cortisol secretion in relation to sleep and wakefulness. Journal of Psychiatry and Neuroscience. 1991;16(2):96-102.
Moreno-reyes R, Kerkhofs M, L’hermite-balériaux M, Thorner MO, Van cauter E, Copinschi G. Evidence against a role for the growth hormone-releasing peptide axis in human slow-wave sleep regulation. Am J Physiol. 1998;274(5 Pt 1):E779-84.
Bes F, Hofman W, Schuur J, Van boxtel C. Effects of delta sleep-inducing peptide on sleep of chronic insomniac patients. A double-blind study. Neuropsychobiology. 1992;26(4):193-7.
Frieboes RM, Murck H, Maier P, Schier T, Holsboer F, Steiger A. Growth hormone-releasing peptide-6 stimulates sleep, growth hormone, ACTH and cortisol release in normal man. Neuroendocrinology. 1995;61(5):584-9.
Kerkhofs M, Van cauter E, Van onderbergen A, Caufriez A, Thorner MO, Copinschi G. Sleep-promoting effects of growth hormone-releasing hormone in normal men. Am J Physiol. 1993;264(4 Pt 1):E594-8.
Peterfi Z, McGinty D, Sarai E, Szymusiak R. Growth hormone-releasing hormone activates sleep regulatory neurons of the rat preoptic hypothalamus. American Journal of Physiology – Regulatory, Integrative and Comparative Physiology. 2010;298(1):R147-R156. doi:10.1152/ajpregu.00494.2009.
Obal F, Jr, Krueger JM. GHRH and sleep. Sleep Med Rev 8: 367– 377, 2004.
Künzel H, Held K, Schmidt D, Ziegenbein M, Murck H, Steiger A. Sleep-endocrine effects of growth hormone-releasing hormone (GHRH) in patients with schizophrenia. J Psychiatr Res. 2018;101:1-4.
Ehlers C, Reed TK, Henriksen SJ. Effects of corticotropin-releasing factor and growth hormone-releasing factor on sleep and activity in rats. Neuroendocrinology 42: 467– 474, 1986.
Nistico G, DeSarro GB, Bagetta G, Müller EE. Behavioural and electrocortical spectrum power effects of growth hormone releasing factor in rats. Neuropharmacology 26: 75– 78, 1987.
Obal F, Jr, Alfoldi P, Cady AB, Johannsen L, Sary G, Krueger JM. Growth hormone-releasing factor enhances sleep in rats and rabbits. Am J Physiol Regul Integr Comp Physiol 255: R310– R316, 1988.
Kerkhofs M, Van CE, Van OA, Caufriez A, Thorner MO, Copinschi G. Sleep-promoting effects of growth hormone-releasing hormone in normal men. Am J Physiol Endocrinol Metab 264: E594– E598, 1993.
Marshall L, Molle M, Boschen G, Steiger A, Fehm HL, Born J. Greater efficacy of episodic than continuous growth hormone-releasing hormone (GHRH) administration in promoting slow-wave sleep (SWS). J Clin Endocrinol Metab 81: 1009– 1013, 1996.
Steiger A, Guldner J, Hemmeter U, Rothe B, Wiedemann K, Holsboer F. Effects of growth hormone-releasing hormone and somatostatin on sleep EEG and nocturnal hormone secretion in male controls. Neuroendocrinology 56: 566– 573, 1992.
Takahashi Y, Kipnis DM, Daughaday WH. Growth hormone secretion during sleep. J Clin Invest 47: 2079– 2090, 1968.
Tannenbaum GS, Martin JB. Evidence for an endogenous ultradian rhythm governing growth hormone secretion in the rat. Endocrinology 98: 562– 570, 1976.
Kimura F, Tsai CW. Ultradian rhythm of growth hormone secretion and sleep in the adult male rat. J Physiol (Lond) 353: 305– 315, 1984.
Mitsugi N, Kimura F. Simultaneous determination of blood levels of corticosterone and growth hormone in the male rat: relation to sleep-wakefulness cycle. Neuroendocrinology 41: 125– 130, 1985.
Bruhn TO, Anthony EL, Wu P, Jackson IM. GRF immunoreactive neurons in the paraventricular nucleus of the rat: an immunohistochemical study with monoclonal and polyclonal antibodies. Brain Res 424: 290– 298, 1987.
Steiger A. Sleep and endocrine regulation. Front Biosci 8: s358– s376, 2003.
Zhang J, Obal F, Jr, Zheng T, Fang J, Taishi P, Krueger JM. Intrapreoptic microinjection of GHRH or its antagonist alters sleep in rats. J Neurosci 19: 2187– 2194, 1999.
Baker LD, Barsness SM, Borson S, et al. Effects of growth hormone–releasing hormone on cognitive function in adults with mild cognitive impairment and healthy older adults: results of a controlled trial. Arch Neurol. 2012;69(11):1420-9.
Vitiello MV, Moe KE, Merriam GR, Mazzoni G, Buchner DH, Schwartz RS. Growth hormone releasing hormone improves the cognition of healthy older adults. Neurobiol Aging. 2006;27(2):318-23.
Friedman SD, Baker LD, Borson S, et al. Growth Hormone–Releasing Hormone Effects on Brain γ-Aminobutyric Acid Levels in Mild Cognitive Impairment and Healthy Aging. JAMA neurology. 2013;70(7):883-890. doi:10.1001/jamaneurol.2013.1425.
Baker LD, Vitiello MV. Growth hormone-releasing hormone improves cognitive function in older adults: sleep on it–reply. JAMA Neurol. 2013;70(4):529-30.
Available at https://www.alzforum.org/news/research-news/growth-hormone-releasing-hormone-slows-cognitive-decline-mci.
Growth hormone-releasing hormone improves the cognition of healthy older adults. Neurobiol Aging. 2006 Feb;27(2):318-23.
Dou Y, Zhang Q, Zhang X, Dong JY, Tang JJ, et al. (2009) Effect of different immunomodulation on inflammatory response in burn rats with sepsis. Zhonghua Shao Shang Za Zhi CHN 25: 275–280.
Isgaard J, Aberg D, Nilsson M (2007) Protective and regenerative effects of the GH/IGF-I axis on the brain. Minerva Endocrinol ITA 32: 103–113.
Vitiello MV, Moe KE, Merriam GR, Mazzoni G, Buchner DH, Schwartz RS. Growth hormone releasing hormone improves the cognition of healthy older adults. Neurobiol Aging. 2006;27(2):318–323.
Zhang H, Han M, Zhang X, Sun X, Ling F. The Effect and Mechanism of Growth Hormone Replacement on Cognitive Function in Rats with Traumatic Brain Injury. Ferreira ST, ed. PLoS ONE. 2014;9(9):e108518. doi:10.1371/journal.pone.0108518.
Pathipati P, Surus A, Williams CE, Scheepens A (2009) Delayed and chronic treatment with growth hormone after endothelin-induced stroke in the adult rat. Behav Brain Res NED 204: 93–101.
Ying XG, Wu BC, Zhang YM, Shao JH (2004) Recombinant human growth hormone on acute effects of coronary collateral circulation in rats with myocardial infarction. J Clin Cardiovascu Dis CHN 10: 613–615.
Christophidis LJ, Gorba T, Gustavsson M, Williams CE, Werther GA, et al. (2009) Growth hormone receptor immunoreactivity is increased in the subventricular zone of juvenile rat brain after focal ischemia: a potential role for growth hormone in injury-induced neurogenesis. Growth Horm Igf Res SCO 19: 497–506.
Koutkia P, Canavan B, Breu J, Grinspoon S. Effects of growth hormone-releasing hormone on bone turnover in human immunodeficiency virus-infected men with fat accumulation. J Clin Endocrinol Metab. 2005;90(4):2154-60.
Clemmesen B, Overgaard K, Riis B, Christiansen C. Human growth hormone and growth hormone releasing hormone: a double-masked, placebo-controlled study of their effects on bone metabolism in elderly women. Osteoporos Int. 1993;3(6):330-6.
Holloway L, Butterfield G, Hintz RL, Gesundheit N, Marcus R. Effects of recombinant human growth hormone on metabolic indices, body composition, and bone turnover in healthy elderly women. J Clin Endocrinol Metab. 1994;79:470–479. doi: 10.1210/jcem.79.2.7519191.
Kruse HP, Kuhlencordt F. On an attempt to treat primary and secondary osteoporosis with human growth hormone. Horm Metab Res Horm Stoffwechselforschung Horm Métabolisme. 1975;7:488–491. doi: 10.1055/s-0028-1093710.
Brixen K, Kassem M, Nielsen HK, Loft AG, Flyvbjerg A, Mosekilde L. Short-term treatment with growth hormone stimulates osteoblastic and osteoclastic activity in osteopenic postmenopausal women: a dose response study. J Bone Miner Res Off J Am Soc Bone Miner Res. 1995;10:1865–1874. doi: 10.1002/jbmr.5650101205.
Clemmesen B, Overgaard K, Riis B, Christiansen C. Human growth hormone and growth hormone releasing hormone: a double-masked, placebo-controlled study of their effects on bone metabolism in elderly women. Osteoporos Int J Establ Result Coop Eur Found Osteoporos Natl Osteoporos Found USA. 1993;3:330–336.
Erdtsieck RJ, Pols HA, Valk NK, van Ouwerkerk BM, Lamberts SW, Mulder P, Birkenhäger JC. Treatment of post-menopausal osteoporosis with a combination of growth hormone and pamidronate: a placebo controlled trial. Clin Endocrinol (Oxf) 1995;43:557–565.
Holloway L, Kohlmeier L, Kent K, Marcus R. Skeletal effects of cyclic recombinant human growth hormone and salmon calcitonin in osteopenic postmenopausal women. J Clin Endocrinol Metab. 1997;82:1111–1117. doi: 10.1210/jcem.82.4.3901.
Joseph F, Ahmad AM, Ul-Haq M, Durham BH, Whittingham P, Fraser WD, Vora JP. Effects of growth hormone administration on bone mineral metabolism, PTH sensitivity and PTH secretory rhythm in postmenopausal women with established osteoporosis. J Bone Miner Res Off J Am Soc Bone Miner Res. 2008;23:721–729. doi: 10.1359/jbmr.071117.
Kassem M, Brixen K, Mosekilde L, Blum WF, Flyvbjerg A. Effects of growth hormone treatment on serum levels of insulin-like growth factors (IGFs) and IGF binding proteins 1-4 in postmenopausal women. Clin Endocrinol (Oxf) 1998;49:747–756.
Kassem M, Brixen K, Blum WF, Mosekilde L, Eriksen EF. Normal osteoclastic and osteoblastic responses to exogenous growth hormone in patients with postmenopausal spinal osteoporosis. J Bone Miner Res Off J Am Soc Bone Miner Res. 1994a;9:1365–1370. doi: 10.1002/jbmr.5650090907.
Kassem M, Brixen K, Blum W, Mosekilde L, Eriksen EF. No evidence for reduced spontaneous or growth-hormone-stimulated serum levels of insulin-like growth factor (IGF)-I, IGF-II or IGF binding protein 3 in women with spinal osteoporosis. Eur J Endocrinol Eur Fed Endocr Soc. 1994b;131:150–155.
Landin-Wilhelmsen K, Nilsson A, Bosaeus I, Bengtsson BA. Growth hormone increases bone mineral content in postmenopausal osteoporosis: a randomized placebo-controlled trial. J Bone Miner Res Off J Am Soc Bone Miner Res. 2003;18:393–405. doi: 10.1359/jbmr.2003.18.3.393.
Sugimoto T, Nakaoka D, Nasu M, Kanzawa M, Sugishita T, Chihara K. Effect of recombinant human growth hormone in elderly osteoporotic women. Clin Endocrinol (Oxf) 1999;51:715–724.
Kruse HP, Kuhlencordt F. On an attempt to treat primary and secondary osteoporosis with human growth hormone. Horm Metab Res Horm Stoffwechselforschung Horm Métabolisme. 1975;7:488–491. doi: 10.1055/s-0028-1093710.
Krantz E, Trimpou P, Landin-Wilhelmsen K. Effect of Growth Hormone Treatment on Fractures and Quality of Life in Postmenopausal Osteoporosis: A 10-Year Follow-Up Study. The Journal of Clinical Endocrinology and Metabolism. 2015;100(9):3251-3259. doi:10.1210/jc.2015-1757.
Gillberg P, Mallmin H, Petrén-Mallmin M, Ljunghall S, Nilsson AG. Two years of treatment with recombinant human growth hormone increases bone mineral density in men with idiopathic osteoporosis. J Clin Endocrinol Metab. 2002;87:4900–4906. doi: 10.1210/jc.2002-020231.
Johansson AG, Lindh E, Blum WF, Kollerup G, Sørensen OH, Ljunghall S. Effects of growth hormone and insulin-like growth factor I in men with idiopathic osteoporosis. J Clin Endocrinol Metab. 1996;81:44–48. doi: 10.1210/jcem.81.1.8550792.
Tzanela M. Adult growth hormone deficiency: to treat or not to treat. Expert Opin Pharmacother. 2007;8:787–795. doi: 10.1517/14656566.8.6.787.
Kužma M, Kužmová Z, Zelinková Z, Killinger Z, Vaňuga P, Lazurová I, Tomková S, Payer J. Impact of the growth hormone replacement on bone status in growth hormone deficient adults. Growth Horm IGF Res Off J Growth Horm Res Soc Int IGF Res Soc. 2014;24:22–28. doi: 10.1016/j.ghir.2013.12.001.
Mo D, Fleseriu M, Qi R, Jia N, Child CJ, Bouillon R, Hardin DS. Fracture risk in adult patients treated with growth hormone replacement therapy for growth hormone deficiency: a prospective observational cohort study. Lancet Diabetes Endocrinol. 2015;3:331–338. doi: 10.1016/S2213-8587(15)00098-4.
Schmidmaier G, Wildemann B, Heeger J, et al. Improvement of fracture healing by systemic administration of growth hormone and local application of insulin-like growth factor-1 and transforming growth factor-beta1. Bone. 2002;31(1):165-72.
Alba M, Fintini D, Sagazio A, et al. Once-daily administration of CJC-1295, a long-acting growth hormone-releasing hormone (GHRH) analog, normalizes growth in the GHRH knockout mouse. Am J Physiol Endocrinol Metab. 2006;291(6):E1290-4.
Barake M, Arabi A, Nakhoul N, et al. Effects of growth hormone therapy on bone density and fracture risk in age-related osteoporosis in the absence of growth hormone deficiency: a systematic review and meta-analysis. Endocrine. 2018;59(1):39-49.
Gillberg P, Mallmin H, Petrén-mallmin M, Ljunghall S, Nilsson AG. Two years of treatment with recombinant human growth hormone increases bone mineral density in men with idiopathic osteoporosis. J Clin Endocrinol Metab. 2002;87(11):4900-6.
Krantz E, Trimpou P, Landin-wilhelmsen K. Effect of Growth Hormone Treatment on Fractures and Quality of Life in Postmenopausal Osteoporosis: A 10-Year Follow-Up Study. J Clin Endocrinol Metab. 2015;100(9):3251-9.
Kuzma M, Payer J. [Growth hormone deficiency, its influence on bone mineral density and risk of osteoporotic fractures]. Cas Lek Cesk. 2010;149(5):211-6.
Vittorio Locatelli and Vittorio E. Bianchi, “Effect of GH/IGF-1 on Bone Metabolism and Osteoporsosis,” International Journal of Endocrinology, vol. 2014, Article ID 235060, 25 pages, 2014.
Capozzi A, Casa SD, Altieri B, Pontecorvi A. Low bone mineral density in a growth hormone deficient (GHD) adolescent. Clinical Cases in Mineral and Bone Metabolism. 2013;10(3):203-205.
Aloia JF, Zanzi I, Ellis K, et al. Effects of growth hormone in osteoporosis. J Clin Endocrinol Metab. 1976;43(5):992-9.
Bolanowski M, Halupczok J, Jawiarczyk-Przybyłowska A. Pituitary Disorders and Osteoporosis. International Journal of Endocrinology. 2015;2015:206853. doi:10.1155/2015/206853.
Sugimoto T, Kaji H, Nakaoka D, et al. Effect of low-dose of recombinant human growth hormone on bone metabolism in elderly women with osteoporosis. Eur J Endocrinol. 2002;147(3):339-48.
The Endocrine Society. “Growth hormone reduces risk of osteoporosis fractures in older women: Long-term follow-up study shows benefits lasted for years after randomized trial.” ScienceDaily. ScienceDaily, 27 August 2015. <www.sciencedaily.com/releases/2015/08/150827141905.htm>.
Holmes D. Bone: Antifracture efficacy of growth hormone-confirmation at long last. Nat Rev Endocrinol. 2015;11(11):631.
Balercia G, Giovannini L, Paggi F, Spaziani M, Tahani N, Boscaro M, Lenzi A, Radicioni A. GH deficiency in the transition period: body composition and gonad function. J Endocrinol Invest. 2011 Jun 21.
Ohlsson C, Bengtsson BA, Isaksson OG, Andreassen TT, Slootweg MC. Growth hormone and bone. Endocr Rev. 1998 Feb;19(1):55–79.
Bex M, Bouillon R. Growth hormone and bone health. Horm Res. 2003;60( Suppl 3):80–6.
Groban L, Lin M, Kassik KA, Ingram RL, Sonntag WE. Early-onset growth hormone deficiency results in diastolic dysfunction in adult-life and is prevented by growth hormone supplementation. Growth Horm IGF Res. 2011 Apr;21(2):81–8. Epub 2011 Mar 2.
Isaksson OG, Ohlsson C, Bengtsson BA, Johannsson G. GH and bone-experimental and clinical studies. Endocr J. 2000 Mar;47( Suppl):S9–16.
Li Y, Chen LQ, Liang L. Effects of recombinant human growth hormone (GH) replacement therapy on bone metabolism in children with GH deficiency. Zhejiang Da Xue Xue Bao Yi Xue Ban. 2005 Jul;34(4):312–5.
Binnerts A, Swart GR, Wilson JH, Hoogerbrugge N, Pols HA, Birkenhager JC, Lamberts SW. The effect of growth hormone administration in growth hormone deficient adults on bone, protein, carbohydrate and lipid homeostasis, as well as on body composition. Clin Endocrinol (Oxf) 1992 Jul;37(1):79–87.
Boot AM, van der Sluis IM, Krenning EP, de Muinck Keizer-Schrama SM. Bone mineral density and body composition in adolescents with childhood-onset growth hormone deficiency. Horm Res. 2009;71(6):364–71. Epub 2009 Jun 9.
Shea HC, Levy RA. Transition Care of Growth Hormone Deficient Patients from Pediatric Endocrinologists to Adult Endocrinologists. Endocr Pract. 2011 Nov;8:1–34.
Wüster C., Abs R., Bengtsson B.-A., et al. The influence of growth hormone deficiency, growth hormone replacement therapy, and other aspects of hypopituitarism on fracture rate and bone mineral density. Journal of Bone and Mineral Research. 2001;16(2):398–405. doi: 10.1359/jbmr.2001.16.2.398.
Mazziotti G., Bianchi A., Bonadonna S., et al. Increased prevalence of radiological spinal deformities in adult patients with GH deficiency: influence of GH replacement therapy. Journal of Bone and Mineral Research. 2006;21(4):520–528. doi: 10.1359/jbmr.060112.
Akaltun İ, Çayır A, Kara T, Ayaydın H. Is growth hormone deficiency associated with anxiety disorder and depressive symptoms in children and adolescents?: A case-control study. Growth Horm IGF Res. 2018;41:23-27.
Nicholas LM, Tancer ME, Silva SG, Underwood LE, Stabler B. Short stature, growth hormone deficiency, and social anxiety. Psychosom Med. 1997;59(4):372-5.
Stabler B. Impact of growth hormone (GH) therapy on quality of life along the lifespan of GH-treated patients. Horm Res. 2001;56 Suppl 1:55-8.
Stabler B, Clopper RR, Siegel PT, et al. Links between growth hormone deficiency, adaptation and social phobia. Horm Res. 1996;45(1-2):30-3.
Brod M, Pohlman B, Højbjerre L, Adalsteinsson JE, Rasmussen MH. Impact of adult growth hormone deficiency on daily functioning and well-being. BMC Research Notes. 2014;7:813. doi:10.1186/1756-0500-7-813.
Wexler T, Gunnell L, Omer Z, et al. Growth Hormone Deficiency Is Associated with Decreased Quality of Life in Patients with Prior Acromegaly. The Journal of Clinical Endocrinology and Metabolism. 2009;94(7):2471-2477. doi:10.1210/jc.2008-2671.
Mahajan T, Crown A, Checkley S, Farmer A, Lightman S. Atypical depression in growth hormone deficient adults, and the beneficial effects of growth hormone treatment on depression and quality of life. Eur J Endocrinol. 2004;151:325–332. doi: 10.1530/eje.0.1510325.
Malik IA, Foy P, Wallymahmed M, Wilding JP, MacFarlane IA. Assessment of quality of life in adults receiving long-term growth hormone replacement compared to control subjects. Clin Endocrinol (Oxf) 2003;59:75–81. doi: 10.1046/j.1365-2265.2003.01799.x.
Stouthart PJ, Deijen JB, Roffel M, HA D-v d W. Quality of life of growth hormone (GH) deficient young adults during discontinuation and restart of GH therapy. Psychoneuroendocrinology. 2003;28:612–626. doi: 10.1016/S0306-4530(02)00045-8.
McMillan CV, Bradley C, Gibney J, Healy ML, Russell-Jones DL, Sonksen PH. Psychological effects of withdrawal of growth hormone therapy from adults with growth hormone deficiency. Clin Endocrinol (Oxf) 2003;59:467–475. doi: 10.1046/j.1365-2265.2003.01870.x.
Koltowska-Haggstrom M, Mattsson AF, Monson JP, Kind P, Badia X, Casanueva FF, Busschbach J, Koppeschaar HP, Johannsson G. Does long-term GH replacement therapy in hypopituitary adults with GH deficiency normalise quality of life. Eur J Endocrinol. 2006;155:109–119. doi: 10.1530/eje.1.02176.
Dahl RE, Birmaher B, Williamson DE, et al. Low growth hormone response to growth hormone-releasing hormone in child depression. Biol Psychiatry. 2000;48(10):981-8.
Deijen JB, De boer H, Blok GJ, Van der veen EA. Cognitive impairments and mood disturbances in growth hormone deficient men. Psychoneuroendocrinology. 1996;21(3):313-22.
Peabody CA, Warner MD, Markoff E, Hoffman AR, Wilson DM, Csernansky JG. Growth hormone response to growth hormone releasing hormone in depression and schizophrenia. Psychiatry Res. 1990;33(3):269-76.
Baker LD, Barsness SM, Borson S, et al. Effects of Growth Hormone–Releasing Hormone on Cognitive Function in Adults With Mild Cognitive Impairment and Healthy Older Adults: Results of a Controlled Trial. Archives of neurology. 2012;69(11):1420-1429. doi:10.1001/archneurol.2012.1970.
Krishnan KR, Manepalli AN, Ritchie JC, et al. Growth hormone-releasing factor stimulation test in depression. Am J Psychiatry. 1988;145(1):90-2.
Steiger A, Guldner J, Colla-müller M, Friess E, Sonntag A, Schier T. Growth hormone-releasing hormone (GHRH)-induced effects on sleep EEG and nocturnal secretion of growth hormone, cortisol and ACTH in patients with major depression. J Psychiatr Res. 1994;28(3):225-38.
Burman P, Hetta J, Wide L, Månsson JE, Ekman R, Karlsson FA. Growth hormone treatment affects brain neurotransmitters and thyroxine [see comment]. Clin Endocrinol (Oxf). 1996;44(3):319-24.
Dinan TG. Psychoneuroendocrinology of depression. Growth hormone. Psychiatr Clin North Am. 1998;21(2):325-39.
Barth C, Villringer A, Sacher J. Sex hormones affect neurotransmitters and shape the adult female brain during hormonal transition periods. Frontiers in Neuroscience. 2015;9:37. doi:10.3389/fnins.2015.00037.
Brigitta B. Pathophysiology of depression and mechanisms of treatment. Dialogues in Clinical Neuroscience. 2002;4(1):7-20.
Terry LC, Crowley WR, Johnson MD. Regulation of Episodic Growth Hormone Secretion by the Central Epinephrine System: STUDIES IN THE CHRONICALLY CANNULATED RAT. Journal of Clinical Investigation. 1982;69(1):104-112.
Nyberg F. Growth hormone in the brain: characteristics of specific brain targets for the hormone and their functional significance. Front Neuroendocrinol. 2000;21(4):330-48.
Available at https://link.springer.com/chapter/10.1007/978-1-4684-5505-2_8.
Ghigo E, Arvat E, Bellone J, Ramunni J, Camanni F. Neurotransmitter control of growth hormone secretion in humans. J Pediatr Endocrinol. 1993;6(3-4):263-6.
Martin JB. Functions of central nervous system neurotransmitters in regulation of growth hormone secretion. Fed Proc. 1980;39(11):2902-6.
Brod M, Pohlman B, Højbjerre L, Adalsteinsson JE, Rasmussen MH. Impact of adult growth hormone deficiency on daily functioning and well-being. BMC Research Notes. 2014;7:813. doi:10.1186/1756-0500-7-813.
Maggi M, Buvat J, Corona G, Guay A, Torres LO. Hormonal causes of male sexual dysfunctions and their management (hyperprolactinemia, thyroid disorders, GH disorders, and DHEA). J Sex Med. 2013;10(3):661-77.
Ginzburg E, Lin A, Sigler M, Olsen D, Klimas N, Mintz A. Testosterone and growth hormone normalization: a retrospective study of health outcomes. Journal of multidisciplinary healthcare. 2008;1:79-86.
Brod M, Højbjerre L, Adalsteinsson JE, Rasmussen MH. Assessing the impact of growth hormone deficiency and treatment in adults: development of a new disease-specific measure. J Clin Endocrinol Metab. 2014;99(4):1204-12.
Available at https://www.researchgate.net/publication/12600670_Effects_of_growth_hormone_on_male_reproductive_functions.
Galdiero M, Pivonello R, Grasso LF, Cozzolino A, Colao A. Growth hormone, prolactin, and sexuality. J Endocrinol Invest. 2012;35(8):782-94.
Becker AJ, Uckert S, Stief CG, et al. Possible role of human growth hormone in penile erection. J Urol. 2000;164(6):2138-42.
Becker AJ, Uckert S, Stief CG, et al. Serum levels of human growth hormone during different penile conditions in the cavernous and systemic blood of healthy men and patients with erectile dysfunction. Urology. 2002;59(4):609-14
Otunctemur A, Ozbek E, Sahin S, et al. Low serum insulin-like growth factor-1 in patients with erectile dysfunction. Basic and Clinical Andrology. 2016;26:1. doi:10.1186/s12610-015-0028-x.
Rajfer J. Growth Factors and Gene Therapy for Erectile Dysfunction. Reviews in Urology. 2000;2(1):34.
Pastuszak AW, Liu JS, Vij A. IGF-1 levels are significantly correlated with patient-reported measures of sexual function. International journal of impotence research. 2011; 23(5):220-6.
Pastuszak AW, Liu JS, Vij A, et al. IGF-1 levels are significantly correlated with patient-reported measures of sexual function. Int J Impot Res. 2011;23(5):220-6.
El-Sakka AI, Lin CS, Chui RM, Dahiya R, Lue TF. Effects of diabetes on nitric oxide synthase and growth factor genes and protein expression in an animal model. Int J Impot Res. 1999;11:123–32. doi: 10.1038/sj.ijir.3900392.
Soh J, Katsuyama M, Ushijima S, Mizutani Y, Kawauchi A, Yabe-Nishimura C, et al. Localization of increased insulin-like growth factor binding protein-3 in diabetic rat penis: Implications for erectile dysfunction. Urology. 2007;70:1019–23. doi: 10.1016/j.urology.2007.07.057.
Pu XY, Zheng XG, Zhang Y, Xiao HJ, Xu ZP, Liu JM, et al. Higher expression of mRNA and protein of insulin-like growth factor binding protein-3 in old rat penile tissues: implications for erectile dysfunction. J Sex Med. 2011;8:2181–90. doi: 10.1111/j.1743-6109.2011.02318.x.
Khorram O, Laughlin GA, Yen SS. Endocrine and metabolic effects of long-term administration of [Nle27]growth hormone-releasing hormone-(1-29)-NH2 in age-advanced men and women. J Clin Endocrinol Metab. 1997;82(5):1472-9.
Rubinek T, Rubinfeld H, Hadani M, Barkai G, Shimon I. Nitric oxide stimulates growth hormone secretion from human fetal pituitaries and cultured pituitary adenomas. Endocrine. 2005;28(2):209-16.
Valverde I, Peñalva A, Ghigo E, Casanueva FF, Dieguez C. Involvement of nitric oxide in the regulation of growth hormone secretion in dogs. Neuroendocrinology. 2001;74(4):213-9.
Rigamonti AE, Cella SG, Marazzi N, Müller EE. Nitric oxide modulation of the growth hormone-releasing activity of Hexarelin in young and old dogs. Metab Clin Exp. 1999;48(2):176-82.
Doi SQ, Jacot TA, Sellitti DF, et al. Growth hormone increases inducible nitric oxide synthase expression in mesangial cells. J Am Soc Nephrol. 2000;11(8):1419-25.
Available at http://erj.ersjournals.com/content/31/4/815.
Deniz Tuncel, Fatma Inanc Tolun, and Ismail Toru, “Serum Insulin-Like Growth Factor-1 and Nitric Oxide Levels in Parkinson’s Disease,” Mediators of Inflammation, vol. 2009, Article ID 132464, 4 pages, 2009.
Available at https://clinicaltrials.gov/ct2/show/NCT00470002.
Böger RH , Skamira C , Bode-Böger SM , Brabant G , von zur Muhlen A , Frolich JC. 1996. Nitric oxide may mediate the hemodynamic effects of recombinant growth hormone in patients with acquired growth hormone deficiency. A double-blind, placebo-controlled study. J Clin Invest 98:2706–2713.
Thum T , Fleissner F , Klink I , Tsikas D , Jakob M , Bauersachs J , Stichtenoth DO. 2007. Growth hormone treatment improves markers of systemic nitric oxide bioavailability via insulin-like growth factor-I. J Clin Endocrinol Metab 92:4172–4179.
Mani maran RR, Sivakumar R, Ravisankar B, et al. Growth hormone directly stimulates testosterone and oestradiol secretion by rat Leydig cells in vitro and modulates the effects of LH and T3. Endocr J. 2000;47(2):111-8.
Ho KY, Evans WS, Blizzard RM, et al. Effects of sex and age on the 24-hour profile of growth hormone secretion in man: importance of endogenous estradiol concentrations. J Clin Endocrinol Metab. 1987;64(1):51-8.
Bancroft J. The endocrinology of sexual arousal. J Endocrinol. 2005;186(3):411-27.
Alwaal A, Breyer BN, Lue TF. Normal male sexual function: emphasis on orgasm and ejaculation. Fertility and sterility. 2015;104(5):1051-1060. doi:10.1016/j.fertnstert.2015.08.033.
Andersson KE. Mechanisms of penile erection and basis for pharmacological treatment of erectile dysfunction. Pharmacol Rev. 2011;63:811–59.
Dail WG, Moll MA. Localization of vasoactive intestinal polypeptide in penile erectile tissue and in the major pelvic ganglion of the rat. Neuroscience. 1983;10:1379–86.
Yasui Y, Saper CB, Cechetto DF. Calcitonin gene-related peptide (CGRP) immunoreactive projections from the thalamus to the striatum and amygdala in the rat. J Comp Neurol. 1991;308:293–310.
Hedlund P, Ekström P, Larsson B, Alm P, Andersson KE. Heme oxygen-ase and NO-synthase in the human prostate—relation to adrenergic, cholinergic and peptide-containing nerves. J Auton Nerv Syst. 1997;63:115–26.
Jen PY, Dixon JS, Gosling JA. Co-localization of nitric oxide synthase, neuropeptides and tyrosine hydroxylase in nerves supplying the human postnatal vas deferens and seminal vesicle. Br J Urol. 1997;80:291–9.
King SH, Mayorov AV, Balse-Srinivasan P, Hruby VJ, Vanderah TW, Wessells H. Melanocortin Receptors, Melanotropic Peptides and Penile Erection. Current topics in medicinal chemistry. 2007;7(11):1098-1106.
Wessells H, Blevins JE, Vanderah TW. Melanocortinergic control of penile erection. Peptides. 2005;26(10):1972–7.
Wessells H, et al. Synthetic melanotropic peptide initiates erections in men with psychogenic erectile dysfunction: double-blind, placebo controlled crossover study. J. Urol. 1998;160(2):389–93.
Zipf WB, Payne AH, Kelch RP. Prolactin, growth hormone, and luteinizing hormone in the maintenance of testicular luteinizing hormone receptors. Endocrinology. 1978;103(2):595-600.
Doessing S, Heinemeier KM, Holm L, et al. Growth hormone stimulates the collagen synthesis in human tendon and skeletal muscle without affecting myofibrillar protein synthesis. The Journal of Physiology. 2010;588(Pt 2):341-351. doi:10.1113/jphysiol.2009.179325.
Bach LA, Hale LJ. Insulin-like growth factors and kidney disease. Am J Kidney Dis. 2015;65:327–336.
Devesa J, Almengló C, Devesa P. Multiple Effects of Growth Hormone in the Body: Is it Really the Hormone for Growth? Clinical Medicine Insights Endocrinology and Diabetes. 2016;9:47-71. doi:10.4137/CMED.S38201.
Scheepens A, Williams CE, Breier BH, Guan J, Gluckman PD. A role for the somatotropic axis in neural development, injury and disease. J Pediatr Endocrinol Metab. 2000;13(Suppl 6):1483–1491.
Pathipati P, Gorba T, Scheepens A, Goffin V, Sun Y, Fraser M. Growth hormone and prolactin regulate human neural stem cell regenerative activity. Neuroscience. 2011;190:409–427.
Devesa P, Reimunde P, Gallego R, Devesa J, Arce V. Growth hormone (GH) treatment may cooperate with locally-produced GH in increasing the proliferative response of hippocampal progenitors to kainate-induced injury. Brain Inj. 2011;25:503–510.
David Aberg N, Lind J, Isgaard J, Georg KH. Peripheral growth hormone induces cell proliferation in the intact adult rat brain. Growth Horm IGF Res. 2010;20:264–269.
Aberg ND, Johansson UE, Aberg MA, et al. Peripheral infusion of insulin-like growth factor-I increases the number of newborn oligodendrocytes in the cerebral cortex of adult hypophysectomized rats. Endocrinology. 2007;148:3765–3772.
Pang Y, Zheng B, Fan LW, Rhodes PG, Cai Z. IGF-1 protects oligodendrocyte progenitors against TNF alpha-induced damage by activation of PI3K/Akt and interruption of the mitochondrial apoptotic pathway. Glia. 2007;55:1099–1107.
Gonzalez-Perez O, Alvarez-Buylla A. Oligodendrogenesis in the subventricular zone and the role of epidermal growth factor. Brain Res Rev. 2011;67:147–156.
Pan SN, Ma HM, Su Z, Zhang CX, Zhu SY, Du ML. Epidermal growth factor receptor signaling mediates growth hormone-induced growth of chondrocytes from sex hormone-inhibited adolescent rats. Clin Exp Pharmacol Physiol. 2011;38:534–542.
Sim FJ, Zhao C, Penderis J, Franklin RJ. The age-related decrease in CNS remyelination efficiency is attributable to an impairment of both oligodendrocyte progenitor recruitment and differentiation. J Neurosci. 2002;22:2451–2459.
Longobardi S, Keay N, Ehrnborg C, Cittadini A, Rosen T, Dall R, et al. Growth hormone (GH) effects on bone and collagen turnover in healthy adults and its potential as a marker of GH abuse in sports: a double blind, placebo-controlled study. The GH-2000 Study Group. J Clin Endocrinol Metab. 2000;85:1505–1512.
Powrie JK, Bassett EE, Rosen T, Jorgensen JO, Napoli R, Sacca L, et al. Detection of growth hormone abuse in sport. Growth Horm IGF Res. 2007;17:220–226.
Ueland T, Fougner SL, Godang K, Schreiner T, Bollerslev J. Serum GH and IGF-I are significant determinants of bone turnover but not bone mineral density in active acromegaly: a prospective study of more than 70 consecutive patients. Eur J Endocrinol. 2006;155:709–715.
Dioufa N, Schally AV, Chatzistamou I, et al. Acceleration of wound healing by growth hormone-releasing hormone and its agonists. Proceedings of the National Academy of Sciences of the United States of America. 2010;107(43):18611-18615. doi:10.1073/pnas.1013942107.
Kiaris H, et al. Ligand-dependent and -independent effects of splice variant 1 of growth hormone-releasing hormone receptor. Proc Natl Acad Sci USA. 2003;100:9512–9517.
Kanashiro-Takeuchi RM, et al. Cardioprotective effects of growth hormone-releasing hormone agonist after myocardial infarction. Proc Natl Acad Sci USA. 2010;107:2604–2609.
Granata R, et al. Growth hormone-releasing hormone promotes survival of cardiac myocytes in vitro and protects against ischaemia-reperfusion injury in rat heart. Cardiovasc Res. 2009;83:303–312.
Ludwig B, et al. Agonist of growth hormone-releasing hormone as a potential effector for survival and proliferation of pancreatic islets. Proc Natl Acad Sci USA. 2010;107:12623–12628.
Kiaris H, Schally AV, Armatis P. Direct action of growth hormone-releasing hormone agonist JI-38 on normal human fibroblasts: Evidence from studies on cell proliferation and c-myc proto-oncogene expression. Regul Pept. 2001;96:119–124.
Kiaris H, Schally AV. Decrease in telomerase activity in U-87MG human glioblastomas after treatment with an antagonist of growth hormone-releasing hormone. Proc Natl Acad Sci USA. 1999;96:226–231.
Bellyei S, et al. GHRH antagonists reduce the invasive and metastatic potential of human cancer cell lines in vitro. Cancer Lett. 2010;293:31–40
Schally AV, Comaru-Schally AM. Growth Hormone Secretagogues. In: Bercu BB, Walker RF, editors. Clinical Practice. Dekker, New York: 1998. pp. 131–142.
McAnulty RJ. Fibroblasts and myofibroblasts: Their source, function and role in disease. Int J Biochem Cell Biol. 2007;39:666–671.
Serini G, Gabbiani G. Mechanisms of myofibroblast activity and phenotypic modulation. Exp Cell Res. 1999;250:273–283.
Available at http://www.medicineatmichigan.org/web-exclusives/2016/february/medsport-studies-hgh-acl-repair.
Khorram O, Yeung M, Vu L, Yen SS. Effects of [norleucine27]growth hormone-releasing hormone (GHRH) (1-29)-NH2 administration on the immune system of aging men and women. J Clin Endocrinol Metab. 1997;82(11):3590-6.
Brown PA, Davis WC, Draghia-akli R. Immune-enhancing effects of growth hormone-releasing hormone delivered by plasmid injection and electroporation. Mol Ther. 2004;10(4):644-51.
Botteri FM, Van der Putten H, Wong DF, Sauvage CA, Evans RM. 1987 Unexpected thymic hyperplasia in transgenic mice harboring a neuronal promoter fused with simian virus 40 large T antigen. Mol Cell Biol . 7:3178–3184.
Blazar BR, Brennan CA, Broxmeyer HE, Schultz LD, Vallera DA. 1995 Transgenic mice expressing either bovine growth hormone (bGH) or human GH releasing hormone (hGRH) have increased splenic progenitor cell colony formation and DNA synthesis in vitro and in vivo. Exp Hematol . 22:1397–1406.
Siriani MC, Annibale B, Tagliaferi F, et al. 1992 Modulation of human natural killer activity by vasoactive intestinal polypeptide (VIP) family. VIP, glucagon, and GHRF specifically inhibit NK activity. Regul Pept . 38:79–87.
Clark R. 1997 The somatogenic hormones and insulin-like growth factor-I: stimulators of lymphopoiesis and immune function. Endocr Rev . 18:157–179.
Auernhammer CJ, Strasburger CJ. 1995 Effect of growth hormone and insulin-like growth factor I on the immune system. Eur J Endocrinol . 133:635–645.
Siriani MC, Annibale B, Tagliaferi F, et al. 1992 Modulation of human natural killer activity by vasoactive intestinal polypeptide (VIP) family. VIP, glucagon, and GHRF specifically inhibit NK activity. Regul Pept . 38:79–87.
Mowles TF, Stricker P, Felix AM, Soike KF, Campbell RM. 1991 Effect of human growth hormone-releasing factor and a potent analog on antibody formation in African Green Monkey. Horm Metab Res . 23:530–534.
Rapaport R, Oleske J, Ahdieh H, Solomon S, Delfaus C, Denny T. Suppression of immune function in growth hormone-deficient children during treatment with human growth hormone. J Pediatr. 1986;109(3):434-9.
Meazza C, Pagani S, Travaglino P, Bozzola M. Effect of growth hormone (GH) on the immune system. Pediatr Endocrinol Rev. 2004;1 Suppl 3:490-5.
Weigent DA. Expression of Lymphocyte-derived Growth Hormone (GH) and GH-releasing Hormone Receptors in Aging Rats. Cellular immunology. 2013;282(2):71-78. doi:10.1016/j.cellimm.2013.04.009.
Arlt W, Hewison M. Hormones and immune function: implications of aging. Aging Cell. 2004;3(4):209-16.
Morrhaye G, Kermani H, Legros J-J, et al. Impact of Growth Hormone (GH) Deficiency and GH Replacement upon Thymus Function in Adult Patients. Unutmaz D, ed. PLoS ONE. 2009;4(5):e5668. doi:10.1371/journal.pone.0005668.
Smith TJ. Insulin-Like Growth Factor-I Regulation of Immune Function: A Potential Therapeutic Target in Autoimmune Diseases? Pharmacological Reviews. 2010;62(2):199-236. doi:10.1124/pr.109.002469.
Ge R-T, Mo L-H, Wu R, et al. Insulin-like growth factor-1 endues monocytes with immune suppressive ability to inhibit inflammation in the intestine. Scientific Reports. 2015;5:7735. doi:10.1038/srep07735.
Smith TJ. Insulin-like growth factor-I regulation of immune function: a potential therapeutic target in autoimmune diseases?. Pharmacol Rev. 2010;62(2):199-236.
Smith TJ. Insulin-like growth factor-I regulation of immune function: a potential therapeutic target in autoimmune diseases?. Pharmacol Rev. 2010;62(2):199-236.
Bilbao D, Luciani L, Johannesson B, Piszczek A, Rosenthal N. Insulin-like growth factor-1 stimulates regulatory T cells and suppresses autoimmune disease. EMBO Molecular Medicine. 2014;6(11):1423-1435. doi:10.15252/emmm.201303376.
Spadaro O, Camell C, Bosurgi L, et al. IGF1 shapes the macrophage activation in response to immunometabolic challenge. Cell reports. 2017;19(2):225-234. doi:10.1016/j.celrep.2017.03.046.
Johannesson B, Sattler S, Semenova E, et al. Insulin-like growth factor-1 induces regulatory T cell-mediated suppression of allergic contact dermatitis in mice. Disease Models & Mechanisms. 2014;7(8):977-985. doi:10.1242/dmm.015362.
Chapes SK, Simske SJ, Forsman AD, Bateman TA, Zimmerman RJ. Effects of space flight and IGF-1 on immune function. Adv Space Res. 1999;23(12):1955-64.
Heemskerk VH, Daemen MA, Buurman WA. Insulin-like growth factor-1 (IGF-1) and growth hormone (GH) in immunity and inflammation. Cytokine Growth Factor Rev. 1999;10(1):5-14.
Granata R., Trovato L., Gallo M. P., et al. Growth hormone-releasing hormone promotes survival of cardiac myocytes in vitro and protects against ischaemia-reperfusion injury in rat heart. Cardiovascular Research. 2009;83(2):303–312. doi: 10.1093/cvr/cvp090.
Penna C., Settanni F., Tullio F., et al. GH-releasing hormone induces cardioprotection in isolated male rat heart via activation of RISK and SAFE pathways. Endocrinology. 2013;154(4):1624–1635. doi: 10.1210/en.2012-2064.
Kanashiro-Takeuchi R. M., Szalontay L., Schally A. V., et al. New therapeutic approach to heart failure due to myocardial infarction based on targeting growth hormone-releasing hormone receptor. Oncotarget. 2015;6(12):9728–9739. doi: 10.18632/oncotarget.3303.
Available at http://www.jimmunol.org/content/166/6/4195.
Mora Rodríguez JA, Porchia LM, Camargo F, López-Bayghen E. The use of insulin-like growth factor 1 improved the parameters of the seminogram in a patient with severe oligoasthenoteratozoospermia. SAGE Open Med Case Rep. 2019;7:2050313X19834154. Published 2019 Mar 5. doi:10.1177/2050313X19834154.
Magon N, Agrawal S, Malik S, Babu KM. Growth hormone in the management of female infertility. Indian J Endocrinol Metab. 2011;15 Suppl 3(Suppl3):S246–S247. doi:10.4103/2230-8210.84876.
Volpe A, Coukos G, Barreca A, Giordano G, Artini PG, Genazzani AR. Clinical use of growth hormone-releasing factor for induction of superovulation. Hum Reprod. 1991;6(9):1228-32.
Patient Success Stories



What to expect during your consultation:
- Usually takes 15-30 minutes
- Completely confidential
- No obligation to purchase anything
- We will discuss your symptoms along with your health and fitness goals
- Free post-consult access for any additional questions you may have
Free Consultation
Start Your Journey to a Younger, Healthier You!



Subscribe




Free Consultation
STEPS AWAY FROM A YOUNGER. HEALTHIER YOU!
Call 800-277-4041 for a Free Consultation
What to expect during your consultation:
- Usually takes 15-30 minutes
- Completely confidential
- No obligation to purchase anything
- We will discuss your symptoms along with your health and fitness goals
- Free post-consult access for any additional questions you may have